

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pilomatricoma is a benign neoplasm originating from hair follicle matrix cells. It was first described by Malherbe and Chenantaisare, who termed the disease "epithelioma of Malherbe," as they believed it was derived from the sebaceous glands (12). Pilomatricomas often present as a asymptomatic, solitary, hard, slow-growing subcutaneous massed, and the overlying skin may occasionally have a bluish discoloration (2). Pilomatricomas are not uncommon and are present in 1 out of every 500 skin specimens submitted to pathologists (3).
There have been several reports of pilomatricoma of the adult male breast in the English medical literature but to the best of our knowledge there are no reports of these cases in the Korean medical literature (456). Almost all published case reports have emphasized that pilomatricoma mimics breast cancer.
Here, we present a case involving an adult male with an incidentally discovered slow-growing palpable mass on his left breast that mimicked male breast cancer.
CASE REPORT
A 69-year-old man presented to our hospital because of a painless palpable mass on his left breast, which had been growing slowly for 10 years, but had recently enlarged rapidly.
Upon initial physical examination, the tumor appeared as a 3.7 × 4.0 cm superficial, exophytic, ulcerative, erythematous soft tissue mass on the patient's left upper inner breast. Nothing of clinical interest was noted in the patient's family history.
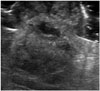
A diagnostic mammogram showed an irregular, exophytic high-density mass with dystrophic calcifications and coarse heterogeneous calcifications (Fig. 1). Ultrasonography showed an irregular, indistinct, exophytic hyperechoic mass at 10 o'clock, 2 cm from the left nipple (Figs. 2, 3). Diffuse skin thickening and soft tissue edema were also present. There were no pathologic lymph nodes in the ipsilateral axilla. These results suggested possible malignancy, and surgical excision was recommended.
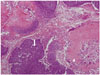
Histologic examination revealed a well-demarcated, nodular, elevated grayish mass with a central ulcer, calcification, and hemorrhage on gross examination. The tumor showed focal necrosis and frequent mitotic figures, but no atypical mitoses were present. A proliferation of basophilic cells and ghost cells was visible under microscopic examination (Fig. 4).
DISCUSSION
Pilomatricoma is the most commonly occurring superficial tumor in children, occurring in about 10% of all resected tissue samples (3). A slight female predominance (female-male ratio, 1.1:1–2.5:1) has been noted (237). The main symptom that presents is a hard, subcutaneous, slow-growing mass with skin discoloration.
The most commonly affected regions are the head and neck, including the preauricular, cheek, and periorbital scalp areas, followed by the upper extremities and trunk (3789). Most head and neck pilomatricomas show varying degrees of calcification and ossification (2).
On the mammogram, the pilomatricoma of the breast was visible as a mass with well-defined margins that contained gross (pleomorphic) calcifications (45610). In this case, dystrophic calcification and coarse heterogeneous microcalcifications were noted. In mammography, pathological breast calcifications are deposits of calcium within the breast tissue. However, the cutaneous calcification present in pilomatricoma is the deposition of insoluble calcium salts in subcutaneous tissue (10).
The ultrasonographic presentation of pilomatricoma is well established. Pilomatricoma typically presents as a well-defined mass with inner echogenic foci and a peripheral hypoechoic rim or a completely echogenic mass with strong posterior acoustic shadowing in the subcutaneous layer (9). In our case, the features found on the sonograph fit the latter case of typical pilomatricoma (heterogeneous hyperechoic mass with focal acoustic shadowing).
Generally, histopathology is required to make a true diagnosis of pilomatricoma. Histopathologically, the tumor is composed of irregularly shaped islands of epithelial cells, which contain basaloid cells, eosinophilic keratinized (ghost or shadow) cells, and cells that are transitional between the former two types. Other identifying features include calcification within the shadow cell islands, a foreign-body giant cell reaction with chronic and acute inflammatory cells, and ossification. This case represents an example of the uncommon perforating variety of pilomatricoma. These pilomatricomas are usually located in the reticular dermis and extend into the subcutaneous tissue, superficial papillary locations, and mid-dermis. Transepidermal elimination is one of the characteristics of perforating pilomatricoma. It has been reported that perforating pilomatricomas grow faster than classic pilomatricomas. Most pilomatricomas do not cause clinical complications. The treatment of choice is surgical excision and the recurrence rate is 2–6% (1). Malignant transformation of pilomatricoma (pilomatrix carcinoma) is very rare.
In summary, we suggest that if slow-growing superficial breast masses in the skin and subcutaneous layers present as hypoechoic masses with calcification, pilomatricoma should be included in the differential diagnosis.


 XML Download
XML Download