

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Polysplenia syndrome is a rare congenital anomaly of situs ambiguous associated with multiple spleens and midline location of abdominal organs. During embryogenesis, the spleen plays an important role in the normal development and lateralization of visceral organs. Therefore, anomalies of the spleen are associated with many congenital anomalies of other organs and show wide spectrum of abnormalities in the abdominal organs (12). Abdominal anomalies of polysplenia syndrome include multiple spleens, various visceral anomalies including impaired visceral lateralization, gastrointestinal abnormalities, and inferior vena cava (IVC) interruption (123).
The majority of patients with polysplenia syndrome die before five years of age because of severe cardiac defects and only 5–10% of the patients with a normal heart or minor cardiac defects can survive to adulthood. Therefore, polysplenia syndromes are often incidentally found by multidetector computed tomography (MDCT) or magnetic resonance imaging for the evaluation of other medical diseases in the adults (456). Although polysplenia syndrome has some characteristic radiologic features, these anomalies may not present clinical pathognomonic symptoms. To the patient undergoing an abdominal surgery, the anomaly itself may make the surgery difficult and increase the risk of complications (7).
In this article, we illustrate various anomalies of polysplenia syndrome and focus on abdominal organs by MDCT with three-dimensional reconstruction images. It is important for radiologists to understand these unfamiliar features of polysplenia syndrome and not interpret them as other pathologic disease pro-cesses.
ABDOMINAL ANOMALIES IN POLYSPLENIA SYNDROME
Polysplenia
The spleen develops from within the dorsal mesogastrium and then incisures on the left side of the dorsal mesogastrium to become the initial splenic primordium during the fifth week of embryogenesis. Therefore, it is regarded that failure of fusion of these incisures can lead to multiple spleens (18).
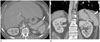
Most patients with polysplenia syndrome have multiple splenic masses of variable size in either left or right side of subphrenic space (Figs. 1, 2) (5). A single lobulated (Fig. 3) and even normal spleens have also been reported (4). The spleens are always located adjacent to the stomach because both the spleen and stomach develop together within the dorsal mesogastrium (18).
Liver, Gallbladder, and Biliary Tract
Pancreas
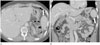
The pancreas may be normal, short in size, or have a cleft created by traversing vessels (2411). An annular pancreas and semiannular pancreas also have been reported (12). A short pancreas may be caused by disease processes such as chronic pancreatitis, ischemic atrophy of the pancreatic tail, Kwashiorkor, and viral infection. In contrast, congenital short pancreas is cau-sed by complete or incomplete agenesis of dorsal pancreas so that only the pancreatic head or pancreatic head with small portion of the pancreas body remains (Fig. 7) (1113). The pancre as head may be located in the midline or right side of midline (Figs. 8, 9). Because both the dorsal pancreas and spleen develop from dorsal mesogastrium, their anomalies tend to occur together (18). Endoscopic retrograde cholangiopancreatography must be performed carefully because the short pancreas may be misdiagnosed as pancreas divisum or mass, which can cause pancreatic duct obstruction. Rarely, a short pancreas can induce pancreatitis due to complete agenesis of the dorsal pancreas may lead to sphincter of Oddi dysfunction or ventral pancreas hyperplasia can give rise to increased pancreatic ductal pressure (14151617).
Gastrointestinal Tract
Malrotation or nonrotation of the gastrointestinal tract is commonly observed in polysplenia syndrome (2318). The stomach may be right-sided, the small bowel may be primarily right-sided and the colon left-sided (Figs. 10, 11), and the cecum may be incompletely fixed (2). Although gastrointestinal tract rotational anomalies may be a rare cause of abdominal pain in adults and may cause bowel obstruction, such as midgut volvulus (318).
IVC Interruption with Azygos or Hemiazygos Continuation
Around the 25th day of embryogenesis, the blood flow of an embryo makes a transition from symmetric to asymmetric. This determines the visceral sidedness. Anomalies of conotruncus and the atrioventricular canal occur at this time (19).
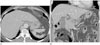
In polysplenia syndrome, some portions of the IVC may be absent because it is primarily a right-sided structure (1). The intrahepatic IVC may be right-sided, left-sided, or duplicated. In the duplicated or right-sided IVC, the IVC is interrupted and connected to the azygos or hemiazygos vein (Fig. 12), whereas, the left-sided IVC is connected to suprahepatic IVC (4). This is the most frequently encountered anatomical anomaly in polysplenia syndrome, albeit not pathognomonic (1245).
Preduodenal Portal Vein
A preduodenal portal vein (PDPV) is a rare anomaly resulting from maldevelopment of portal venous system or malposition of the abdominal viscera. Although PDPV is associated with duodenal atresia, stenosis, web, and annular pancreas; the possibility of duodenal obstruction is low due to its thin wall and low pressure vessel (1111220). PDPV also has been known to cause atrophy of left lateral segment of the liver, selective portal vein obstruction, biliary duct obstruction, long standing malnutrition and cachexia, or toxic and vascular influences (21). PDPV can also give rise to cholelithiasis.
CONCLUSION
Polysplenia syndrome is a rare complex of congenital anomalies characterized by multiple spleens and various visceral anomalies (23). Visceral anomalies of polysplenia syndrome include right-sided stomach, midline or left-sided liver, short pancreas, IVC anomalies, intestinal malrotation, and a PDPV.
MDCT with contrast enhancement and three-dimensional reconstruction is excellent in visualizing these anomalies by providing clear anatomic detail. Because the wide spectrum of anomalies in polysplenia syndrome do not have pathognomonic radiologic features, the knowledge of various radiologic features plays an important role in the diagnosis of this rare syndrome. In addition, correct diagnosis may decrease both the mortality and morbidity under surgical conditions.










 XML Download
XML Download