

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Right colonic diverticulitis is distinctive from left colonic diverticulitis. In Asian populations, unlike Western populations, right colonic diverticulitis is more common than left colonic diverticulitis (12). In right colonic diverticulitis, patients tend to be younger and the inflammation tends to be less extensive (mo-stly limited to a single diverticulum) (234). While left colonic diverticulitis should be clinically differentiated from colon cancer, right colonic diverticulitis is the most frequent alternative diagnosis in patients clinically suspected to have acute appendicitis (56).
In general, a CT scan is essential in diagnosing colonic diverticulitis and classifying the disease severity (7891011). In left colonic diverticulitis, previous studies have consistently showed that a CT scan can be used to determine the need for surgery and to either predict a possible recurrence, or the failure of a non-operative treatment (9111213). In right colonic diverticulitis, however, the precise role of the CT scan has not been established.
We aimed to analyze the need for surgery and recurrence rate using a CT-based method in patients with right colonic diverticulitis.
MATERIALS AND METHODS
Study Overview
The Institutional Review Board approved this retrospective single-center study and waived the informed consent. The study included 416 patients with colonic diverticulitis, with a diagnosis that was based on the findings of a CT scan, and judged by two independent radiologists. These radiologists reviewed the CT images in order to localize the diverticulitis as being right colon, left colon or absent, and to judge the severity of the condition according to the modified Hinchey classification (1014). Two study coordinators (H.J.K. and D.H.K., an abdominal radiologist with 11 years of experience and a radiology resident, respectively) collected the data on the patients' demographics, pre-vious history of colonic diverticulitis, laboratory findings at the time of presentation, patient disposition in regard to surgery, and the recurrence of diverticulitis. Separately, we measured the surgery rate, the recurrence rate, and the severity in patients having right or left colonic diverticulitis using a CT-based method. While right colonic diverticulitis was the main interest of our study, we also collected information on cases of left colonic diverticulitis, in order to compare the two diseases in our population.
Study Sample
The study took place in the Daejin Medical Center Bundang Jesaeng General Hospital-an urban secondary hospital in Korea. Through a computerized search of the hospital's information system, we identified 450 patients who underwent an abdominopelvic CT examination, between January 2010 and August 2013, and then were documented as being diagnosed with colonic diverticulitis. 34 patients were excluded from the study; in these cases, the diagnosis was uncertain, since one of the two radiologists refuted the diagnosis upon reviewing the CT scan images. The remaining 416 patients finally formed the study sample (Fig. 1), with an age of 41.9 ± 13.7 (mean ± standard deviation) deviation) years; of the 416 patients, 238 were men (aged 42.2 ± 12.7 years), and 178 were women (aged 41.4 ± 13.1 years).
The CT Scan Protocol
Intravenous contrast-enhanced portal-venous phase CT examinations were performed, using 16- (Brilliance, Philips, Cleveland, OH, USA) or 64-detector-row machines (Somatom Sensation, Siemens, Forchheim, Germany) (Supplementary Table 1 in the online-only Data Supplement).
Image Interpretation
Two independent radiologists retrospectively reviewed the CT images. While one radiologist (S.K.J., with five years of experience) had been involved in making the original CT reports in some of the patients, the other (K.H.L., with 13 years of clinical experience) was invited from another hospital. Any discrepancies between the two radiologists were resolved by their additional consensus readings. They were familiar with previously reported CT findings of colonic diverticulitis (89101516). They were aware that all patients involved had a final or working diagnosis of colonic diverticulitis; however, any further information on the individual patients was withheld from them. They were asked to localize diverticulitis as being right colon (from the cecum to the proximal half of the transverse colon), left colon (from the distal half of the transverse colon to the sigmoid colon), or absent. They also categorized the severity of diverticulitis according to the modified Hinchey classification adopted from previous studies (1014). Before the interpretation by the two radiologists, to standardize and facilitate the categorization, two abdominal radiologists (H.J.K. and J.W.Y., with 11 and 14 years of clinical experience, respectively) summarized the CT findings for the classification based on previous literature (Table 1) (89101516).
Follow-up
We were able to follow-up 384 of the 416 patients for a median period of 30 months (range, 7-51; interquartile range, 21-38), using a medical record review (n = 332) or telephone interview (n = 52). The remaining 32 patients were deemed unav-ailable for follow-up, as they either did not revisited our hospital nor respond to our telephone calls (n = 31), or they died of concomitant ovarian cancer during the index admission (n = 1).
Clinical Outcomes
The surgery rate was defined as the percentage of patients who underwent any surgical procedure during the index admission or the follow-up period. The surgical procedure included: 1) urgent surgery for patients with diffuse peritonitis, or for those who fail medical treatment, 2) scheduled elective surgery after a cooling-off period of diffuse peritonitis or larger abscess, and 3) prophylactic elective surgery for patients with documented recurrent attack and a relatively young age (at the surgeon's discretion). Recurrence was defined as the presentation of abdominal symptoms and positive findings resulting from CT report after at least one month free of abdominal symptoms following the discharge of the index admission (4).
Statistical Analysis
Interobserver agreement was measured by using the weighted κ statistic (17). Study results were reported for all the patients, and for the subgroups of right and left colonic diverticulitis, separately, focusing on right colonic diverticulitis. The patients with right colonic diverticulitis were further divided into two age groups (under 40 years, and 40 years and above), in order to investigate if there was a debatable difference between the two age groups, with regard to the clinical outcomes of left and right colonic diverticulitis (11). Comparisons were made using the Fisher's exact tests and the Mann-Whitney U-tests. Observed differences were considered significant if the p < 0.05. 95% confidence intervals (CI) were calculated for important percentages, based on a parametric estimate of the standard error for the statistic of interest.
RESULTS
Location of Diverticulitis
For the 34 patients who were excluded from the study by their CT review, the interpretation of the two radiologists is shown in the Supplementary Table 2 (in the online-only Data Supplement). Of the 416 patients who were included in the study, the two radiologists determined that 396 (95.2%) and 20 (4.8%) had diverticulitis in the right and left colon, respectively. No patient had diverticulitis in both.
Interobserver Agreement in Staging
In the 416 patients, the κ value in determining the modified Hinchey classification was 0.82. A discrepancy between the two radiologists occurred in 35 patients, mostly between stages Ia and Ib (n = 32) (Table 2). When the stages Ia and Ib were grouped together, the κ value was 0.96.
In the 396 patients with right colonic diverticulitis, the κ value in determining the modified Hinchey classification was 0.80. A discrepancy between the radiologists occurred in 32 patients, mostly between stages Ia and Ib (n = 30). When the stages Ia and Ib were grouped together, the κ value was 0.96.
Hereinafter, the reported data on the modified Hinchey classification stems from the consensus reading.
Patient Characteristics
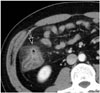
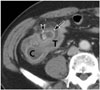
The 396 patients having right colonic diverticulitis included 230 men and 166 women, with a mean age of 41.1 ± 12.6 years. These patients (compared with the 20 patients with left colonic diverticulitis) were younger, had a slightly lower serum C-reactive protein level, and had more cases of lower stages in the modified Hinchey classification (p < 0.001). According to the consensus reading, 98.2% (389/396; 95% CI: 96.9%, 99.5%) of the patients with right colonic diverticulitis had stages Ia-II (Figs. 2, 3), whereas 75% (15/20) of those with left colonic diverticulitis were so (Table 3). Among the patients with right colonic diverticulitis, the subgroup that included those younger than 40 years did not significantly differ from those who were 40 years or older, with regard to the gender, severity, surgery rate, or recurrence rate.
Surgery
Since we were unable to follow-up with 32 of the 416 patients, the surgery rate was calculated using the remaining 384, including 366 and 18 with right and left colonic diverticulitis, respectively (Table 4). Of the 384 patients, 22 underwent surgery and were pathologically confirmed to have diverticulitis. The surgery rate for right colonic diverticulitis [4.6% (17/366); 95% CI: 2.5%, 6.7%] was lower than that for left colonic diverticulitis [28% (5/18)] (p < 0.001).
In the patients with right colonic diverticulitis, surgical procedures included a right hemicolectomy (n = 16) and an ileocecectomy (n = 1). Of the 359 patients with stages Ia-II, 10 (2.8%; 95% CI: 1.1%, 4.5%) patients underwent surgery during the index admission (n = 3) or 3-29 months after the index admission (n = 7). 8 patients underwent surgery for the prevention of a recurrence. Two patients received surgery for the treatment of acute symptoms associated with colonic diverticulitis. All 7 patients of stage III or IV underwent surgery during the index admission for the treatment of acute symptoms (Fig. 4).
In the patients with left colonic diverticulitis, surgical procedures included Hartmann's Procedure (n = 4) and a diverticulectomy from the sigmoid colon (n = 1). Of the 13 patients with stages Ia or Ib, one patient underwent surgery during the index admission for the treatment of acute symptoms. Of the five patients with stages III or IV, 4 patients underwent surgery during the index admission for the treatment of acute symptoms. The remaining one patient with stage IV could not undergo surgery because of poor general condition, and the hospital course was complicated by an intra-abdominal abscess and ileocolic fistula. In other words, there was no serious unresolved complication up to the last follow-up, in the patients with right or left colonic diverticulitis.
Recurrence
47 patients were not included in the calculation of the recurrence rates, since either we were unable to follow-up with them (n = 32), or they had already undergone colonic surgery during the index admission or within one month after the index admission (n = 15). The recurrence rate was 6.5% (23/356; 95% CI: 3.9%, 9.1%) and 15% (2/13) for the patients with right or left colonic diverticulitis, respectively (p = 0.224).
In 356 patients with right colonic diverticulitis with stages Ia-II, 23 (6.5%; 95% CI: 3.9%, 9.1%) had recurrence. The median interval from the discharge of index admission to the recurrence was 4 months (interquartile range, 1-12). Seven of them then underwent surgery in order to prevent further recurrence. The remaining 16 patients were treated medically, without further recurrence up to the last follow-up.
DISCUSSION
With regard to left colonic diverticulitis in Western populations, a CT scan is used to determine the severity of the disease, and the need for surgery (91013). The modified Hinchey classification is the most widely used method to determine the disease severity. In this study, we applied a CT-based modified Hin-chey classification to right colonic diverticulitis in an Asian pop-ulation. We also measured the interobserver agreement of two experienced radiologists, the surgery rate, and the recurrence rate according to the CT-based disease severity. The present study is, to our knowledge, the largest study involving patients with right colonic diverticulitis.
In determining the stage, we observed a fairly high interobserver agreement, showing a kappa value of 0.82. The kappa value was even higher (0.96) when stages Ia and Ib were grouped together; in these cases, differentiation was not likely to be meaningful with respect to the surgery rate and recurrence rate in our results. Importantly, the overwhelming majority (98.2%) of patients with right colonic diverticulitis had lower stages (i.e., Ia-II), rarely in need of surgery (2.8%), and also had a low recurrence rate (6.5%). On the contrary, all seven patients having stage III or IV needed surgery, but our data still had limited precision for patients at stage III or IV due to relatively small sample size.
In our result, stage Ia accounted for 83.8% of our patients with right colonic diverticulitis, who rarely needed surgery (3.3%) and had low recurrence rate (7.0%). These findings corroborate previous smaller studies that advocated non-surgical treatment for patients with right colonic diverticulitis (41819). The uncomplicated disease course in these patients is similar to that of stage Ia of left colonic diverticulitis (2021). Interestingly, our right colonic diverticulitis cases with stage Ib or II (i.e., with a complicating abscess) had a low surgery rate and recurrence rate comparable to those with stage Ia. In left colonic diverticulitis, the CT finding of a complicating abscess (stage Ib or II) has been known to be associated with a high surgery rate (37-59%) and a high recurrence rate (12-19%), and therefore, a colectomy is typically indicated in such cases (91220). Due to the small number of cases of left colonic diverticulitis in our study sample, we were unable to make a formal comparison between right and left colonic diverticulitis by each CT stage.
Our study had limitations. First, our study sample was formed based on the CT findings, since CT is the most accurate (and only practical) test that can establish the diagnosis of colonic diverticulitis. Therefore, cases of very mild diseases which could not be identified by CT (or which did not even need CT) may have been selectively excluded from the study. Had such very mild cases been included, the surgery rate and recurrence rate would have been even lower. Second, the recurrence rate may have been underestimated, as our follow-up period was not very long (median, 30 months). However, the underestimation is likely minute, as recurrent attacks are known to occur mostly in the first year after initial treatment (22).
In conclusion, the CT-based modified Hinchey classification of right colonic diverticulitis showed good interobserver agreement. Most patients with right colonic diverticulitis have lower stages (Ia-II) at CT, who rarely need surgery, and have a low recurrence rate.






 XML Download
XML Download