

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastric adenomyoma is a rare benign subepithelial tumor, characteristically composed of mucosal structures and a prominent smooth muscle stroma (1). The majority of the cases are asymptomatic and are found incidentally during endoscopic examinations, or on computed tomography (CT) scans. However, this disease entity is unfamiliar to endoscopists and radiologists, and it is difficult to diagnose before operation. In this report, we describe a case of a gastric adenomyoma, and present its imaging features.
CASE REPORT
A 28-year-old man with a history of epigastric pain spanning a few days was referred to our hospital for a gastric subepithelial lesion found on the endoscopic examination. His past medical history was unremarkable. A physical examination did not reveal any significant abnormalities. The routine laboratory tests were within the normal ranges.
An endoscopic examination revealed a round mass protruding into the lumen, covered with relatively normal mucosa, in the gastric antrum (Fig. 1). The mass was smoothly compressible by an endoscopic forceps, but an endoscopic biopsy was not conducted. Subsequently, an abdominal CT scan was performed. The CT scan showed a 3.5 cm sized well-circumscribed cystic mass that protruded into the gastric antrum. The lesion had enhancing walls, with uneven thickness, and an internal content of homogeneous density (Fig. 2). No enlarged lymph nodes around the stomach were observed.
A decision for surgical treatment was made for a histologic diagnosis. A laparoscopic wedge resection for the subepithelial mass was performed under general anesthesia.
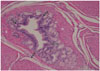
A macroscopic examination revealed a 38 × 35 × 25 mm nodular mass with a yellowish brown color. It was solid and cystic, with clear, mucinous fluid in the lumen. A microscopic examination showed the hypertrophic smooth muscle fibers of the stroma, surrounded by epithelial elements in the form of individual glandular structures (Fig. 3). A final histologic diagnosis was compatible with gastric adenomyoma. The postoperative progress of the patient was uneventful.
DISCUSSION
Adenomyoma of the gastrointestinal tract is a rare benign tumor composed of glands and cysts, lined by columnar, flattened epithelia and a prominent smooth muscle stroma (1). They are most frequently found in the stomach and duodenum (2). In the stomach, the majority of cases involve the distal part of the stomach (antrum 85%, pylorus 15%) (3). The age of the patients at presentation ranges from 1 week to 81 years, and two-thirds of the cases occur in the fourth to sixth decades (34).
Because there are several different opinions on the histogenetic origin, there are various terms used for adenomyomas: myoepithelial hamartoma, myoglandular hamartoma, adenomyomatous hamartoma, and adenomyosis. Several authors have proposed that gastric adenomyoma is considered to be a variant of an ectopic pancreas without exocrine or endocrine components, based on the similarities of the epithelial components (1). Takeyama et al. (5) placed more weight on the abnormal smooth muscle proliferation and considered it to be an hamartoma, resulting from an abnormal interaction between the endoderm- and mesoderm-derived tissues.
Some previously reported cases of gastric adenomyoma demonstrated CT findings, which were identical to the findings in our case, including a well-circumscribed and mainly cystic subepithelial mass that protrudes into the lumen and has irregular or uneven wall thickness (67). The cystic portion of the lesions is correlated with the mucinous component, on the histopathologic examination. Although these findings are nonspecific for subepithelial lesions of the stomach, a differential diagnosis can be narrowed down to several cystic subepithelial lesions: duplication cysts, gastritis cystic profunda and Brunner's gland hyperplasia. Solid subepithelial tumors that can undergo cystic degeneration, such as gastrointestinal stromal tumor and schwannoma can also show similar CT features.
Upon an endoscopic examination, the adenomyoma showed a round bulging mass with overlying normal mucosa that occasionally had central umbilication or ulceration (6). An endoscopic biopsy of the lesion is not useful because the lesions are usually located in the submucosa (1). Recently, endoscopic submucosal dissection has widely been used for subepithelial tumors, and can be the alternative choice for diagnosis and treatment (8).
Although gastric adenomyoma is usually asymptomatic, or has nonspecific symptoms, some complications or symptoms can occur, including localized peritonitis, melena, and gastric outlet obstruction (259). Furthermore, a few cases associated with adenocarcinoma have been reported (3). The relationship between adenomyoma and adenocarcinoma remains unclear. However, the possibility of the malignant transformation of adenomyoma is suggested.
As mentioned above, because of rarity of gastric adenomyoma, non-specific CT and endoscopic findings and uncertain result of endoscopic biopsy, it is difficult to differentiate adenomyoma before operation. Therefore, surgical excision is performed for histologic diagnosis in most cases. During operation, frozen sections are useful for intraoperative diagnosis and avoiding unnecessary radical operation (2). No recurrence after a successful surgical resection has been reported.
In summary, an adenomyoma is a rare subepitheial tumor of the stomach that shows nonspecific CT features. It resembles several diseases, including duplication cysts, gastritis cystica profunda, Brunner's gland hyperplasia and solid tumors with cystic degeneration, in radiologic findings. So, adenomyoma could be included in the differential diagnosis of gastric cystic subepithelial masses, especially in the distal part of the stomach.


 XML Download
XML Download