

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bone wax has been widely used in craniofacial surgery to mechanically control bleeding from bone surfaces and cut edges, since it was introduced to the filed of surgery by Victor Horsley in 1892 (1). Bone wax acts as a molding tamponade, providing a mechanical barrier to hemorrhage. It is inert, pliable, and sturdy enough to fill bony defects; however, it is minimally resorbable and may induce inflammatory reactions, interfere with bone healing, and increase infection rates (2).
Several case reports have described symptomatic complications that developed after the use of bone wax to control bleeding in craniofacial surgery (345678). But, to our knowledge, rarely have there been patients in orbital surgical series that presented with complications due to the use of bone wax (5), and only a small number of reports have described the features of bone wax as detected on CT and MRI (346). Here, we describe the imaging features of bone wax in a patient with clinically diagnosed chronic rhinosinusitis after a dacryocystorhinostomy.
CASE REPORT
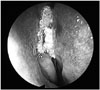
A 71-year-old man presented with a purulent nasal discharge with a foul odor and obstruction after having undergone a dacryocystorhinostomy one year earlier. During this procedure, bone wax had been used to control bleeding from the lacrimal bone. Endoscopic examination revealed a whitish, mass-like lesion in the right anterior upper nasal cavity around the upper attached part of the middle turbinate, as well as a right lacrimal bone defect adjacent to the lacrimal sac (Fig. 1).
CT and MRI scans were then obtained to evaluate this sinonasal lesion. CT revealed a lesion of about the density of fat [about -70 Hounsfield units (HU)] filling the right anterior upper nasal cavity and lacrimal bone defect (Fig. 2). The nasolacrimal duct remained patent but was slightly compressed by the lesion. MRI showed a hypointense or signal-void lesion on all sequences with no contrast enhancement after gadolinium injection (Fig. 3). Differential diagnosis included surgical or packing materials, dermoid cyst, and entrapped orbital fat tissue.
Endoscopic sinus surgery was performed, and a whitish foreign body was found at the right middle meatus. It was removed by forceps and clarified as the bone wax that had been applied during the dacryocystorhinostomy. A pathological examination revealed chronic inflammation of the nasal mucosa, fragmented chondroid, and calcified materials (Fig. 4).
DISCUSSION
The development of modern bone wax has been attributed to Horsley in 1892 (1). It is a hemostatic and sealant agent that is smeared across bleeding edges of bone surfaces to block holes and cause immediate bone hemostasis through a tamponade effect. It is a sterile and opaque mixture of 85 to 90% white beeswax and 10 to 15% isopropyl palmitate, a wax-softening agent, with or without pure paraffin wax (2).
CT attenuation by bone wax generally falls between the low attenuation of fat and the intermediate attenuation of water (4), which we observed by imaging a lump of bone wax floating in a cup of water (Fig. 2D). With the appropriate window settings, CT can clearly discriminate air, bone wax, and surgical instruments, but it might be difficult to differentiate bone wax from lesions consisting of adipose tissue, such as lipomas, dermoid cysts, and entrapped fat tissue. MRI can be used to exclude such lesions based on their high signal intensities on T1-weighted images and intermediate signal intensities on T2-weighted images.
Bone wax is a semicrystalline, solid substance with a very short T2 value. Because it does not generate a signal detectable by means of conventional MRI techniques, bone wax imaging results in a signal void or one of low intensity on all MRI sequences. This characteristic is typical of all crystalline materials, such as ice crystals (9). In our experiment, we observed this signal void on MRI sequences by imaging a lump of bone wax floating in a cup of water (Fig. 3D, E). Signal voids on postoperative MRI can reflect a variety of materials, such as entrapped air, the presence of packing materials, and surgical instruments or other artifacts; however, the signal voids in such cases can be differentiated from those due to bone wax based on their geometry and location. In addition, magnetic susceptibility artifacts generated by paramagnetic surgical instruments have characteristic bright signal margins that are not seen with bone wax because its magnetic permeability is similar to that of water and soft tissue.
Although bone wax is generally a safe material, it can cause chronic inflammation, act as a mechanical barrier to bone regeneration, impair bacterial clearance in cancellous bone, and precipitate the formation of a foreign-body granuloma (2). Complications related to the use of bone wax have been reported in several types of craniofacial operations (34567810).
In 1994, Allison (10) reported foreign-body reactions to bone wax applied in mandibular surgery, including histological findings such as infiltration of lymphocytes, macrophages, and giant cell infiltration. This author also proposed that a foreign-body reaction may be related to the amount of bone wax used and would occur more readily when bone wax is used in a large area.
A year later, Hadeishi et al. (4) described seven cases in which bone wax had migrated to the sigmoid sinus after retromastoid craniectomy. Postoperative CT scans revealed hypodensities (-34 to -79 HU) in the ipsilateral sigmoid sinus indicating the presence of bone wax. They concluded that application of a large quantity of wax to control bleeding from the large emissary veins could risk such migration.
In 1996, Katz and Rootman (5) noted bone wax granulomas of the orbit as a remote surgical complication in two patients and suggested that the wax may indeed act as a nidus for infection and may induce chronic granulomatous giant-cell foreign-body inflammation.
As reported by Kamide et al. (8) in 2009, bone wax-induced osteohypertrophy presented as exophthalmos 9 years after a craniotomy. It is thought that osteohypertrophy is caused by chronic foreign body-induced inflammation that eventually extends into the bone marrow, resulting in osteoblast activation and osteogenesis.
Excess bone wax may have a mass effect. If it obstructs the natural ostium, it can cause acute paranasal sinusitis. Kim et al. (7) described recurrent acute frontal sinusitis caused by bone wax used in a frontal lobe operation. The authors proposed that obstruction of the natural ostium can induce stasis of secretions and ciliary dysfunction and can impair the clearance of bacteria from the paranasal sinus. Similarly, in our patient, excess bone wax may have blocked the drainage pathway from the anterior ostiomeatal complex, leading to chronic rhinosinusitis.
The presence of bone wax can cause complications both immediately after craniofacial surgery and later. Thus, it is important to consider the possible presence of bone wax in postoperative MRI examinations so that it is not mistaken for residual air, surgical instruments, or artifacts. The careful evaluation of bone wax as detected on CT and MRI may allow this differentiation.



 XML Download
XML Download