

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cervical spondylolysis is a rare condition defined as a corticated cleft between the superior and inferior articular facets of the articular pillar (123). Multilevel spondylolysis (4%) is uncommon (345). Bilateral involvement occurs in up to two-thirds of cases (2). To the best of our knowledge, this is the first report of two consecutive levels of unilateral cervical spondylolysis on opposite sides.
CASE REPORT
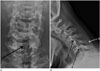
A 19-year-old male visited our hospital complaining of having had neck pain for 3 years, which had been aggravated after a motor vehicle accident 2 years previously. The patient did not complain about sensory abnormality. Motor examination revealed normal bilateral upper extremity strength. Spurling's foraminal compression test was negative on both sides. To evaluate the cause of the neck pain, radiographs of the cervical spine (anteroposterior, lateral, and flexion-extension views) were taken. The anteroposterior radiograph (Fig. 1A) revealed spina bifida of the C5 vertebra, and the lateral flexion radiograph (Fig. 1B) showed two well-defined vertical spondylolytic defects that divided the articular pillars of the C5 and C6 vertebra into two fragments. The flexion-extension views did not show any instability. He was further investigated using computed tomography (CT) and magnetic resonance imaging (MRI) modalities. Axial CT scans (Fig. 2) showed well-corticated defects in the right articular pillar of C5 and the left articular pillar of C6, with irregular shaped ossification in the defect of the left C6 articular pillar. A spina bifida of C5 and ipsilateral dysplastic laminae of C5 and C6 were also noted. Reformatted sagittal CT images on the right side revealed dysplasia of the inferior articular process of C4 and superior articular process of C6. On the left side, dysplasia of the inferior articular process of C5 and superior articular process of C7 were also found. Three-dimensional volume rendering CT images were helpful in the visualization and clarification of the abnormalities. MRI (Fig. 3) showed clefts similar to those seen on CT, and demonstrated no evidence of spinal cord compression or signal abnormality, discoligamentous structure injury, or bone marrow edema. By the combination of described imaging features of radiography, CT, and MRI, and the chronicity of the symptoms, congenital two-level unilateral cervical spondylolysis involving opposite sides was diagnosed. The patient underwent conservative treatment with intermittent analgesic medication and physical therapy. He had relief of pain after 2 months.
DISCUSSION
Cervical spondylolysis is a corticated cleft between the superior and inferior articular facets of the articular pillar, which is considered to be the cervical equivalent of the lumbar spinal pars interarticularis defect (126). Cervical spondylolysis is usually found incidentally after a minor trauma or from the report of chronic neck pain (4). However, patients with cervical spondylolysis who experience a minor trauma have a higher risk of developing neurological impairment compared with patients without cervical spondylolysis (56).
The exact etiology of cervical spondylolysis is not yet clearly understood. Several explanations have been suggested, including congenital, developmental, microtrauma, and post-traumatic nonunion with pseudoarthrosis (256). One common explanation is that this anomaly is caused by impaired ossification within one ossification center (13567). Frequent association with other anomalies, such as spina bifida and articular dysplasia, supports these congenital or developmental theories (23567). Morvan et al. (8), proposed that cervical spondylolysis occurred due to repetitive microtrauma, which results in stress fractures to the pars region. Another explanation is that the dysplastic spine is more susceptible to trauma or stress and leads to spondylolysis (25).
Cervical spondylolysis manifests at various ages between 20 months to 81 years old (125). Due to the function of C6 as a transitional vertebra, it is the most commonly affected level (74%), followed by C4 and C5 (1234568). Cervical spondylolysis has been reported to occur at any level except for C1 (2). Only one case of cervical spondylolysis at C7 has been reported (3). Cervical spondylolysis occurs more frequently in men than in women (male:female = 2:1) (236), and left side involvement is more frequent in unilateral lesions (2). Bilateral involvement occurs in up to two-thirds of cases (24). Most patients have single level involvement and multilevel involvement is uncommon (4%) (23459). Dysplastic posterior elements such as hypoplastic facets and dysplastic changes in adjoining facets are frequent findings (246). In approximately 60% of cases, associated spina bifida is seen (26).
Characteristic radiological features of cervical spinal spondylolysis were reported by Forsberg et al. (1). The features are as follows: a well-marginated cleft between the facets, a triangular configuration of the pillar fragments on either side of the spondylolytic defect, posterior displacement of the dorsal triangular pillar fragment, hypoplasia of the ipsilateral pedicle, spina bifida at the involved level, and compensatory hyper- or hypoplasia of the ipsilateral articular pillars at the level above and/or below the defect (1). CT scans can confirm the exact bony structures including the corticated spondylolytic defect and associated dysplastic and degenerative changes of the affected articular pillar (12). In particular, three-dimensional volume-rendered CT is helpful for differentiation from an acute fracture, because it produces delicate images of the lesion's sclerotic margins. In this case, imaging features of radiography and CT are concordant with findings of cervical spondylolysis. Moreover, in this case, CT shows two irregular-shaped ossifications in the defect of the left C6 articular pillar, and we considered that it may be due to faulty ossification of one of the ossification centers of the C6 articular pillar, or perhaps C7 (10). MRI is useful in assessing the acuteness of the injury by the presence of tissue and bony edema around the involved segment and the cord (23457), and is also helpful in evaluating associated disc prolapse in the unstable segment (2457).
The major differential diagnoses of cervical spondylolysis are traumatic interfacet dislocation and facet fracture-dislocation (3456). Several findings such as smooth and well-corticated margins and associated congenital anomalies favor primary spondylolysis (345). The presence of associated dysplastic changes in the ipsilateral pedicles and laminae is the most important point that favors a diagnosis of cervical spondylolysis (36). In our case, although his trauma history may have led to misdiagnosis, the correct diagnosis of congenital spondylolysis could be made due to definite image findings.
The treatment of cervical spondylolysis depends on symptoms, instability, and neurological deficit (34). Most patients with cervical spondylolysis are treated conservatively (236), however, surgical management of cervical spondylolysis is directed by the segmental instability or failure of conservative therapy (256).
In conclusion, cervical spondylolysis is a rare condition, and this case is the first report of two-level unilateral cervical spondylolysis on opposite sides. The accurate diagnosis of cervical spondylolysis can be made by a thorough review of the medical history and current image findings. Knowledge and a strong suspicion of this condition is essential for physicians and radiologists to avoid potential misdiagnosis and inappropriate management.


 XML Download
XML Download