

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A papillary thyroid microcarcinoma (PTMC) is defined by the World Health Organization as a carcinoma measured at 1.0 cm or less in its greatest dimension (1). There is an increase in the proportion of PTMC identified among all differentiated thyroid carcinomas mainly due to the improvement and increased in use of ultrasound (US) examination, fine-needle aspiration biopsy, and other diagnostic procedures (2). It is estimated that PTMC accounts for up to 30% of all papillary thyroid cancers, although marked geographic differences in incidence rates have been noted (3). In South Korea, PTMC was reported in up to 50.2% of thyroid carcinomas (4). Currently, there is controversy on the extent of surgery necessary for PTMC. In published clinical guidelines of organizations including the American Thyroid Association, the National Comprehensive Cancer Network, and the British Thyroid Association, the general recommendation in cases of lymphadenopathy is to perform lymph node dissection of the affected compartments. In patients with biopsy-proven metastatic lateral cervical lymphadenopathy, therapeutic lateral neck compartmental lymph node dissection was recommended with total thyroidectomy (TT) to provide clearance of disease (5, 6, 7, 8). Patients with preoperatively detected lateral neck node metastasis are more likely to develop recurrence in the lymph nodes (9). Thus, preoperative US examination is important for evaluating lateral metastatic lymph nodes to determine the extent of operation in potentially aggressive PTMC.
Previous studies have reported the usefulness of preoperative US in detecting the presence of clinically apparent cervical lymph node metastasis (9, 10, 11). Ito et al. (9) reported that preoperative US could detect 39% of metastases among patients with pathologically confirmed lateral lymph node metastasis. However, no report has described whether there are any characteristic or dominant imaging features of metastatic lymph nodes in PTMC in comparison with those of papillary thyroid macrocarcinomas. Therefore, this study retrospectively reviewed the sonographic features of metastatic lymph nodes in PTMC compared to papillary thyroid macrocarcinomas and determined whether there were any dominant findings of lateral metastatic lymph nodes in PTMC. Additionally, this study investigated the sonographic features of metastatic lymph nodes limited to the central neck in PTMC and papillary thyroid macrocarcinoma.
MATERIALS AND METHODS
Subjects
From January 2009 through May 2012, 676 patients with pathologically confirmed papillary thyroid carcinoma (PTC) were identified by the Institutional Review Board. None of these patients had undergone previous operation on the head or neck. All patients underwent US before surgery.
Ultrasound Examination
Thyroid US was performed using a 5- to 12-MHz linear transducer (iU22; Philips Healthcare, Bothell, WA, USA) by one radiologist with ten years of experience. When US examination was performed for detecting metastatic lymph nodes, the radiologist was unaware of cytologic confirmation of malignancy in the thyroid masses. The US examinations included both thyroid lobes and all neck levels (I-VI).
Tumor Size
Patients were placed into two groups depending on the size of the tumor. Patients placed in the PTMC group (n = 306) had tumors with a maximum diameter of 10 mm, and those placed in the papillary thyroid macrocarcinoma group (n = 370) had tumors greater than a minimum diameter of 1 cm. A total of 87 patients from the PTMC group and 186 patients from the papillary thyroid macrocarcinoma group were selected because they were suspected of metastatic lymph nodes based on US examination.
Image Evaluation
The US features of metastatic lymph nodes of the total 273 patients were reviewed by two radiologists. The following US criteria were used to define lymph node metastasis: round shape (minor axis greater than 50% of major axis), loss of fatty hilum, focal or diffuse hyperechogenicity, cystic change, and microcalcification (12, 13, 14). Initially, we compared US features of metastatic lymph nodes in the lateral neck of patients with PTMC and those of patients with papillary thyroid macrocarcinoma. Subsequently, the US features of metastatic lymph nodes in the central neck were reviewed.
Lymph Nodes
Based on findings of US examinations, patients were classified into two groups: the first group had only central neck node (level VI) metastasis; the second group had metastases extended to the lateral neck node (levels II-V). The definition of cervical compartment used in this study was based on the rules outlined by the Head and Neck Service of the Memorial Sloan-Kettering Cancer Center (15, 16).
Of the 186 patients with papillary thyroid macrocarcinoma, 90 were suspected of only central neck node metastasis, whereas 96 were suspected of central and lateral neck node metastasis. Of the 87 patients with PTMC, 58 were suspected of only central neck node metastasis, while 29 were suspected of central and lateral neck node metastasis.
Cytopathologic Evaluation
Lateral neck node metastasis was confirmed by Nodal fine-needle aspiration biopsy (FNAB) or Nodal FNAB needle-wash thyroglobulin (Tg). Nodal FNAB needle-wash Tg measurements could complement cytology in thyroid cancer because it has been reported that these measurements could be used as diagnostic substitute (17, 18). All thyroid tumors and lymph node metastases were confirmed as PTC by pathologic examination. In addition, lymph node metastases were identified by levels. Radiologic findings of suspected lymph node metastasis were correlated with the pathologic evaluation findings.
Surgical Procedure
Patient flow diagram is shown in Fig. 1. All patients underwent routinely TT with central compartment neck dissection. Modified radical neck dissection (MRND) of the affected side was performed for patients diagnosed with extended lateral neck node metastasis (PTMC, n = 29; papillary thyroid macrocarcinoma, n = 96).
Statistical Analysis
Statistical analysis was performed using the chi-square test and a Fisher's exact test. Statistical calculations were performed using the statistical package SPSS for Windows, released in 20.0.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was considered when p value was less than 0.05.
RESULTS
Patients
Of the 273 patients suspected of metastatic lymph nodes based on the US examination, 231 (84.6%) were women, 42 (15.4%) were men. The mean age was 45 years (range, 19-81 years).
Ultrasound Features of Metastatic Lymph Nodes
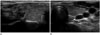
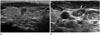
The US features of metastatic lymph nodes in PTMC and papillary thyroid macrocarcinoma are summarized in Table 1. The following diagnostic results were found in the papillary thyroid macrocarcinoma group: round shape (central vs. lateral neck node metastasis: n = 86, 95.6% vs. n = 70, 72.9%), loss of hilum (n = 29, 32.2% vs. n = 84, 87.5%), hyperechogenicity (n = 14, 15.6% vs. n = 87, 90.6%), cystic change (n = 12, 13.3% vs. n = 32, 33.3%), and calcification (n = 2, 2.2% vs. n = 20, 20.8%). For the PTMC group, the following results were obtained: round shape (central vs. lateral neck node metastasis: n = 54, 93.1% vs. n = 19, 65.5%), loss of hilum (n = 12, 20.7% vs. n = 26, 89.7%), hyperechogenicity (n = 8, 13.8% vs. n = 27, 93.1%), cystic change (n = 4, 6.9% vs. n = 9, 31%), and calcification (n = 1, 1.7% vs. n = 7, 24.1%) (Figs. 2, 3, 4, 5).
Of the 125 patients suspected of lateral neck node metastasis, no significant difference of US features was found between the microcarcinoma (n = 96) and macrocarcinoma (n = 29) groups as shown in Figs. 4 and 5. The following analysis was made based on image findings: round shape (microcarcinoma vs. macrocarcinoma: n = 19, 65.5% vs. n = 70, 72.9%, p = 0.221), loss of hilum (n = 26, 89.7% vs. n = 84, 87.5%, p = 0.556), hyperechogenicity (n = 27, 93.1% vs. n = 87, 90.6%, p = 0.555), cystic change (n = 9, 31.0% vs. n = 32, 33.3%, p = 0.533), calcification (n = 7, 24.1% vs. n = 20, 20.8%, p = 0.435). The frequency of lateral neck node metastasis in papillary thyroid macrocarcinoma (52%) was significantly (p = 0.020) higher than that in PTMC (33%) (Table 2). There was significant difference of frequency in PTMC between central neck node (n = 58) and lateral neck node (n = 29) metastases, with p < 0.001 for loss of hilum, hyperechogenicity, cystic change, and calcification. Similar results were obtained for the papillary thyroid macrocarcinoma group with p < 0.001 for loss of hilum, hyperechogenicity, cystic change, and calcification. The round shape was the more frequent finding than other four variables in central neck node metastasis in both papillary thyroid macrocarcinoma group and PTMC group, with p < 0.001 for loss of hilum, hyperechogenicity, cystic change, and calcification (Table 3).
DISCUSSION
Currently research has indicated that thyroid cancer is the most common endocrine malignancy. PTC is the most frequent histological subtype, accounting for 80% of all cases. Increasing global interest in this disease partially stems from the increasing number of its diagnoses. Several authors have demonstrated that the incidence of PTC has almost doubled over the last three decades, mainly due to the higher incidence of PTMC (19, 20). This increase is attributable to the widespread use of cervical ultrasound and ultrasound-guided fine-needle aspiration biopsies of thyroid nodules as well as more accurate histopathological search for small PTMC (19, 21).
In spite of the overall excellent prognosis for patients with PTMC, there is a 1.0% disease-related mortality rate, 5.0% lymph node recurrence rate, and 2.5% distant metastasis rate associated with PTMC. In addition, PTMC has been highly associated with lymph node metastasis at the time of diagnosis, with incidence rate up to 26.3% (22). The presence of lymph node metastasis is an important prognostic factor that indicates the potential for an increasing rate of distant metastasis and the risk of cervical lymph node recurrence (3). Many factors such as tumor mutifocality, bilaterality, capsule invasion, and size (> 5 mm) have been proposed as risk factors of cervical lymph node metastasis in PTMC. These factors are the same for individuals with papillary thyroid macrocarcinoma (22, 23, 24). Some studies have demonstrated that distinguishing PTMC from conventional PTC based on size alone may be erroneous because the recurrence rates for PTMC and conventional PTC are not significantly different. In fact, both tumors behave similarly (25). Some authors have demonstrated that the ipsilateral lateral compartment was involved almost as often as the central compartment (24, 26, 27, 28). However, currently no report has compared any characteristic or dominant imaging features of metastatic lymph nodes in PTMC with papillary thyroid macrocarcinomas. The results from this study indicated that there were no significant difference in US features of metastatic lymph nodes between PTMC and papillary thyroid macrocarcinomas. Not only relatively high incidence of lymph node metastasis, but also all features of metastatic lymph nodes were well presented in PTMC examination. Treatment of patients with PTMC has been suggested to be similar to treatment of patients with conventional PTC (3, 29). Given the relatively low sensitivity of US in evaluating potential metastatic lymph nodes in the central neck, it is reasonable to consider a prophylactic central neck dissection with a total thyroidectomy or lobectomy, even when clear US evidence for local metastatic disease is absent. It is reasonable to consider a therapeutic central neck dissection based on intraoperative findings of positive nodal metastases in this region. Cervical nodal metastases are quite common in PTC. Initial nodal metastasis in PTC usually occurs in the paratracheal and pretracheal nodes in level VI of the central compartment of the ipsilateral neck (26). Preoperative B-Raf proto-oncogene analysis by FNAB based on US may assist the prediction of occult central neck lymph node metastasis in patients with PTC. Previous studies have used indications of clinically node-negative neck and tumor size > 5 mm as predictive factors for subclinical central lymph node metastasis in PTMC (30, 31). Many trials have used it to predict and detect central metastasis. However, the characteristic US features of central metastatic lymph nodes have not yet been demonstrated. Therefore, the US features of metastatic central neck lymph nodes were reviewed in this study to determine if there were any dominant findings that could be used clinically for central neck lymph node examinations. Our results indicated that round shape was the most frequent finding in central neck node metastasis of both PTMC and papillary thyroid macrocarcinomas. This might be due to the relatively low sensitivity of US in evaluating potential metastatic lymph nodes in the central neck. A considerably high percentage of small lesions might have led to the difficulty in identifying inner structures and any changes of lesions. Our findings also indicated that the possibility of metastasis might be suspected when the central lymph node exhibited only round shape.
This study had several limitations. First, only patients suspected of lateral neck node metastasis based on US and those who had undergone surgery with pathologically confirmed metastasis were included, which might have selection bias. However, based on research findings, MRND is not necessary nor recommended for patients without definite lateral neck node metastasis detected on preoperative US. This was because lymph node recurrence-free survival rates did not differ between patients who underwent MRND and patients who did not undergo MRND if there was no preoperative detection of lateral neck node metastasis. In addition, research has shown that, in more than 60% of patients, latent lymph node metastasis only occasionally becomes clinically apparent that requires treatment (9). Finally, this study analyzed only central neck nodes detected with US, which may cause selection bias. To overcome these limitations, further studies are needed to assess the findings using large study groups.
In conclusion, there was no significant difference in US findings of metastatic LNs between the PTMC and the papillary thyroid macrocarcinoma groups, although the frequency of lateral neck node metastasis in the macrocarcinoma group was higher than in the PTMC group. Therefore, it is recommended that careful evaluation of metastatic lymph nodes should be conducted, even if only microcarcinoma is present in the thyroid gland.






 XML Download
XML Download