

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Epithelioid sarcoma is an uncommon, slow-growing soft tissue tumor that usually arises in the distal part of an upper extremity, predominantly occuring in young adults. In magnetic resonance imaging (MRI), an epithelioid sarcoma usually appears as a subcutaneous mass or ulcer with cutaneous erosion (1, 2, 3). MRI appearance with the unusual manifestations of epithelioid sarcoma, such as an intraarticular tumor (1, 4), a subcu-taneous honeycomb pattern (3), periosteum or bone involvement mimicking a primary intraosseous tumor (5, 6), is evolving. However, manifestation as abscesses without a discrete mass is extremely rare (5). Here, we report a 68-year-old patient with unusual image findings and an unusual clinical manifestation for classic-type epithelioid sarcoma in the lower leg. Without an apparent mass, the lesion manifested as numerous small disseminated intramuscular droplet-like nodules with ring-enhancement, mimicking abscesses in the entire lower leg.
Case Report
A 68-year-old male farmer presented with swelling and pain in his left lower leg. Symptoms had developed approximately 6 months previously, and included hearing a popping sound from his left lower leg while working. After 3 months, the pain increased in intensity, becoming almost continuous, and was combined with severe swelling of the calf area, and disabled him from his normal daily work.
Physical examination showed diffuse swelling and tenderness from the knee to the ankle joint. The lower leg showed an erythematous change, with no other accompanying skin changes such as ulceration. No detectable warmth was noted, and the knee and ankle joint demonstrated a full range of motion despite the pain. Other musculoskeletal examinations were noncontributory. On laboratory assessment, the complete blood cell count, the erythrocyte sedimentation rate and the C-reactive protein were normal, and there was no evidence of prolongation of prothrombin time or activated partial thromboplastin time to suspect bleeding tendency. Based on clinical history and examination, the orthopedic surgeon suspected muscle strain with hematoma.
Imaging findings of a plain radiograph of the left lower leg were interpreted as severe soft tissue swelling without evidence of fracture or abnormal periosteal reaction at the tibia and fibula. MRI was performed subsequently without delay. Fat-suppressed T2-weighted imaging demonstrated numerous disseminated about small, droplet-like nodular lesions with hyperin-tense signal (roughly 1 cm in diameter), mainly in the superficial and deep posterior compartments of the lower leg (Fig. 1A, C). The nodules were oval or ellipsoid in shape, and in few were found internal intermediate or low signal foci (Fig. 1C). The margins of the nodules were thin, of relatively regular thickness, with some of them having a low signal intensity rim (Fig. 1A, C). On the contrast enhanced image, the majority of these nodular lesions showed peripheral ring-like enhancement (Fig. 1B, D). Diffuse muscular signal changes were combined with focal fluid collection posterior to the tibialis posterior. These muscular signal changes and nodular lesions were also noted in the anterior compartment of the leg. Diffuse concentric subcutaneous edema was noted. These findings were present along the entire scanned area of the lower leg from the proximal tibia to the tibiotalar joint. There was no evidence of a dominant mass or hematoma. The bone marrow signal alteration was not noted. Tendons, vessels, knee and ankle were considered normal. Imaging findings were interpreted as a multifocal complicated fluid collection with muscular strain.
The patient received an incisional biopsy at the calf. At surgery, discharge without a dominant mass was noted. Histologically, there were round-to-polygonal shaped epithelioid cells with abundant eosinophilic cytoplasm and atypical nuclei possessing vesicular chromatin and small nucleoli (Fig. 2A). Immunohistochemically, the epithelioid cells were positive for cytokeratin (Fig. 2B) and CD34 (Fig. 2C) with a complete loss of INI1 protein expression (Fig. 2D). Histological findings were compatible with classic-form epithelioid sarcoma.
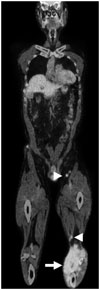
For tumor staging, the patient underwent positron emission tomography/CT and a chest CT, which showed ipsilateral popliteal, inguinal and external iliac metastatic lymph nodes (Fig. 3), and multiple lung metastases (Fig. 4). There were also focal fluorodeoxyglucose (FDG) uptakes at the very caudal part of the tibia and fibula suggesting bone metastases that were not fully revealed in the initial lower leg MRI. Focal FDG uptake was also noted at the left ilium.
Treatment was based on a combination of chemotherapy and palliative radiation therapy. No significant tumoral improvement was noted at the 2-month and 4-month follow-up visits by a lower leg MRI. Instead, hematogenous lung metastases increased in number, size, and extent in every follow-up as seen by chest CT. Four and a half months after his first visit, the patient was admitted to the hospital for dyspnea. Plain chest radiographs showed increased density with aggravation at each follow-up, performed every one or two days. Physicians suspected a combination of pneumonia. Oxygen saturation decreased with aggravation of dyspnea, and the patient died of his disease 5 months after his first visit.
DISCUSSION
Epithelioid sarcoma is rare and accounts for only 0.6-1% of sarcomas (7). Two clinicopathological subtypes are recognized, the classic (distal)-form and the proximal-type variant. Men show slight predominance for this disease over women at 1.9:1 for the classic-type and 1.6:1 for the proximal-type (7).
Until recently, epithelioid sarcoma was seen to occur most frequently in adolescents and young adults. While this finding is concordant with the classic-subtype, the proximal-type variant tends to affect a somewhat older population, with over 80% of patients presenting between 20 and 65 years of age (7). The patient in our case was 69 years old, which is unusual for presentation with the classic-type.
Epithelioid sarcoma occurs in the distal parts of the extremities. Up to 60% occur in the forearm and hand. The lower extre-mities are the second most common site, accounting for 25% to 32% of cases (7).
The two clinicopathological subtypes have different clinical and histological manifestations. The distal-type, which accounts for twice as many cases as the proximal-type (8), usually shows slow growing painless nodules (7). Tumors of the proximal-type appear to have somewhat more malignant potential and a poorer prognosis (9). Even though, the patient in our case was confirmed histopathologically to have the classic-type, the patient had a 3-month history of progressing pain in the lower leg with multiple bone, lymph node and lung metastases.
The epithelioid sarcoma can begin in both the subcutaneous and deeper tissues. Superficial lesions may elevate above the dermis and ulcerate through the skin surface. These tumors ge-nerally manifest as solitary or multiple nodules. Infiltration may be seen, but tends to be restricted to regions around the primary tumor. Deeper lesions are usually larger and less well defined, and frequently present as soft tissue indurations or as multinodular lumpy masses. Tumors are known to have a tendency to grow along fascial planes, tendon sheaths, and neurovascular bundles, and to involve nerves or large vessels (1, 2, 3, 9). In the case presented here, an apparent mass-like lesion was absent. Direct invasion of large vessels was not noted, however, as a result of hematogenous lung metastases, vascular involvement was highly suspected. In addition, diffuse subcutaneous edema was noted but no skin ulceration was present.
The MRI findings in our case were confusing and unusual for soft tissue sarcoma. The absence of an apparent mass lesion with numerous ring-like enhancing nodules, and a diffuse muscular signal change created diagnostic confusion and precluded recognition of the tumor. Nodules were small and disseminated mainly in the posterior compartment muscles throughout the entire lower leg, combined with cystic changes. Several previous reports refer to infiltration of muscle and soft tissues rather than a tumoral mass (1, 3, 6). However, manifestation as a cystic or necrotic component in MR imaging is rare (2, 3, 5), though a disseminated cystic honeycombed-pattern without a discrete mass, resulting from perineural invasion and lymphatic fibrosis by the tumor was noted in a case reported by Yamato et al. (3). Their patient presented with a cutaneous erosion and ulcer with multiple osteolytic lesions due to cortical invasion by an adjacent soft tissue tumor. Dion et al. (5) also reported an epithelioid sarcoma mimicking an abscess, however, the patient in this case had a roughly 10 cm-sized discrete structure without any signal alteration of subjacent muscle.
In hindsight, we realize that a few rare imaging findings in MRI should have been taken into account in a diagnosis favoring a tumoral condition over a complicated fluid-filled lesion such as an abscess. Since epithelioid sarcoma is known to often show necrosis, nodules with a cystic change and internal intermediate signal foci disseminated in entire lower leg without any sign of infection, should be considered as tumoral necrosis. Propensity to spread along the fascia by undulating bands of cells punctuated by foci of necrosis (7), is observed in epithelioid sarcoma. The nodules in our case were numerous, and were disseminated in distribution, hence interpretation of the spread pattern was not easy, however there were many of located along intermuscular fascia.
Metastases from epithelioid sarcomas develop in approximately 40-50% of cases, with involvement of the lung, lymph nodes and, less frequently, the scalp, adrenal gland and stomach (2, 9). Our patient had a classic-type tumor, showing ipsilateral popliteal, inguinal and external iliac lymph node enlargement with FDG uptake. Additional multiple metastases were noted in the lung and bones. Recent studies of epithelioid sarcoma reported a 5-year survival rate of 60-80% and a 10-year rate of 40-60% (7). Adverse prognostic factors include male gender, older age, proximal extremity/axial location, involvement of deep soft tissue, a tumor size over 5 cm, nodal involvement, and extensive necrosis (7, 10), all of which were seen in our patient. Additional adverse prognostic factors are a high mitotic activity, proximal-type histology with the presence of rhabdoid cells, and a high FNCLCC histological grade (7).
In conclusion, this case demonstrates that classic-type epithelioid sarcoma can present as multiple necrotic disseminated nodular lesions with ring-like enhancement, and can mimic abscesses with the absence of an apparent mass. Therefore, epithelioid sarcoma should be considered as a differential diagnosis with such image findings, without definite evidence of infection signs.



 XML Download
XML Download