

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Unilateral lower limb edema can be caused by several conditions such as deep vein thrombosis (DVT), lymphedema, and chronic venous insufficiency (1). It is necessary to also be aware of the uncommon causes of this condition. We report an unusual case of a patient with unilateral limb edema, which occurred due to a synovial cyst that was treated successfully with surgical intervention.
CASE REPORT
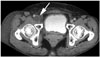
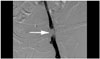
A 52-year-old woman, with diabetes mellitus and a 10-year history of hypertension, presented with a gradually worsening right leg edema without pain which persisted for a month. There was no history of trauma, arthritis, or immobilization. During physical examination, no abnormality was found except for the presence of pitting edema in the right leg. Ultrasonography (US), contrast-enhanced computed tomography (CT), and ascending venography were performed to rule out the DVT. US showed 2.1 cm sized hypoechoic mass compressing the right common femoral vein (Fig. 1). There was no blood flow within the mass on Doppler US. The CT scan demonstrated a 2.3 cm sized homogenous hypodense, well-defined, cystic mass compressing the right common femoral vein in front of the right hip joint (Fig. 2). No deep venous thrombosis was detected in the right lower extremity. Ascending venography was performed to demonstrate extrinsic compression and the absence of clots. It showed filling defect of the right common femoral vein, without the development of collateral venous flow (Fig. 3). On the basis of these findings, differential diagnosis included synovial cyst, ganglion cyst, paralabral cyst, and noninflammatory pseudotumor. During the surgery, a cystic mass of 2.5 cm in size was found protruding from the right hip joint and compressing the posterior wall of the left common femoral vein. The cystic mass was easily separated from the right common femoral vein and was excised successfully. No communication was found between the hip joint space and the cyst. Histological examination confirmed the diagnosis of a synovial cyst (Fig. 4). Surgical removal of the synovial cyst restored normal venous return and promptly relieved the patient's symptoms. The patient was discharged on the fifth postoperative day.
DISCUSSION
Benign cystic lesion, associated with compression of the femoral vein and lower leg edema around the hip joint is a rare condition. Until now, 33 cases have been reported in literature, including this case (2, 3, 4). Histologically, there are two types of cysts: synovial and ganglion cysts. While synovial cyst is a juxta-articular fluid collection lined by synovial cells, ganglion cyst is thought to be a myxomatous degeneration of certain fibrous tissue structures without the lining of synovial cell (3). Since the treatment for these two para-articular cysts is similar, clinical differentiation of ganglion and synovial cysts may not be important. Moreover, distinguishing between synovial and ganglion cyst using imaging is not always possible (5). It is known that synovial cyst is usually accompanied by the conditions affecting the hip, such as rheumatoid arthritis and osteoarthritis (6). A synovial cyst is a herniation of the synovial membrane caused by inflammation with an overproduction of synovial fluid (7). Such a cyst may cause unilateral edema in the lower extremity, when it compresses the adjacent venous structure (2). The most common clinical manifestation of a synovial cyst of the hip joint is a palpable mass or the pain in the inguinal area or in the anterior thigh, due to compression of the femoral nerve (8). Iliopsoas bursitis presents with a triad of findings, which includes a mass in the inguinal region, pressure effect on the nearby structures, and roentgenologic arthritic changes (9). However, Iwata et al. (4) insisted that the presence of an inguinal mass and groin pain is not mandatory for the diagnosis of iliopsoas bursitis. In addition, one report has shown that in only 55% of the cases with a synovial cyst of the hip joint, compression of the adjacent vein was accompanied by a hip joint condition such as rheumatoid arthritis and osteoarthritis (2). Our patient also presented with unilateral edema in the lower leg, without a history of hip joint disease and other clinical manifestations such as pain or the presence of a palpable mass. The mass may have been difficult to palpate and it may not have caused compression of the femoral nerve, because of its small size and location under the femoral vein. Therefore, because a synovial cyst of the hip joint can only cause the lower limb edema without any other symptoms, it should be considered in the differential diagnosis of other conditions such as DVT and lymphedema.
Of the various imaging tools, US may be the most cost-effective, simple, and quick assessment of a synovial cyst in the inguinal area. However, it is difficult to differentiate between a cystic and solid mass, when the cyst contains debris and hyperplastic synovium (10). Although contrast-enhanced CT scan is a suitable imaging modality for the evaluation of the cyst size and its effect on the surrounding structures, magnetic resonance imaging (MRI) is the most accurate imaging technique for assessing the characteristics of soft tissue abnormalities and those associated joint disorders (3). All communications between the iliopsoas bursa and hip joint were demonstrated on MRI, whereas US demonstrated these in only 56% and CT in 60% of the cases (10). Ascending venography is useful for differentially diagnosing the synovial cyst of the hip joint and DVT, and it also helps to avoid anticoagulation therapy. However, recent developments in imaging techniques have decreased the need for venography.
A synovial cyst of the hip joint can be treated by surgical excision, needle aspiration, total hip arthroplasty, or instillation of a steroid or sclerosing agent (2, 4). In asymptomatic cases, it may be left untreated. However, when the vessels or nerves around the inguinal region are compressed by the cyst, it should be surgically excised because of the associated high rate of recurrence (37%) (2).
In conclusion, this case demonstrates that unilateral edema in the lower extremity may be caused by a synovial cyst of the hip joint, without any accompanying arthropathies or symptoms such as pain and a mass in the inguinal region. In the presence of compression of the adjacent vessel or nerve, surgical excision is the treatment of choice for a synovial cyst of the hip joint.


 XML Download
XML Download