

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pathologies of the falciform ligament have rarely been reported (1, 2, 3), and torsion of the lipomatous appendage of the falciform ligament is especially uncommon (4, 5, 6). All the previously reported patients underwent surgical treatment (4, 5, 6), but some reports indicated that segmental omental infarction can be successfully treated conservatively (7, 8). Therefore, surgical treatment can be avoided when torsion of the lipomatous appendage of the falciform ligament is diagnosed accurately.
Herein, we reported the serial ultrasound (US) and computed tomography (CT) findings of torsion of the lipomatous appendage of the falciform ligament that was treated conservatively.
CASE REPORT
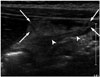
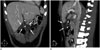
A 13-year-old boy presented with right upper quadrant (RUQ) and epigastric pain during 3 days. Physical examination revealed tenderness in the RUQ without rebound tenderness. Laboratory findings showed elevated aspartate aminotransferase, alanine aminotransferase, and direct and indirect bilirubin (3058 IU/L, 1567 IU/L, 2.2 mg/dL and 1.5 mg/dL, respectively). Neither leukocytosis nor elevated C-reactive protein was noted. The patient was referred to our institution with suspected cholecystitis and hepatitis. Longitudinal US images of the RUQ showed a non-compressible, heterogeneously hyperechoic mass-like lesion at the anterior of the falciform ligament extending along with ligamentum teres (Fig. 1). The lesion did not move with the adjacent intraperitoneal structure during respiration. Maximal tenderness during real-time US was noted just above the lesion. Diffuse gallbladder wall edema was also noted, which was considered as secondary finding due to acute hepatitis. CT images of the upper abdomen on the same day showed about 4.9 × 3.6 × 3 cm heterogeneous, low attenuated mass-like lesion at the anterior of the falciform ligament beneath the rectus abdominis muscle. Coronal and sagittal reformatted CT images showed a close relationship between the lesion and falciform ligament (Fig. 2). The differential diagnosis included torsion of the lipomatous appendage or tumorous condition of the falciform ligament. However, torsion of the lipomatous appendage of the falciform ligament was the preferred diagnosis because neither a cystic nor an enhancing solid mass was noted on US and CT.
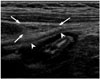
The RUQ pain and tenderness was improved during the 3 day follow-up. On follow-up US, the characteristics of the mass-like lesion was changed to homogeneous hyperechogenicity (Fig. 3). The size of the lesion was slightly decreased, as compared with the previous US finding.
Two weeks later, the RUQ pain and tenderness was completely resolved on physical examination. On a follow-up US, the previous mass-like lesion had almost completely resolved with a scanty amount of fatty tissue remaining at the anterior of the falciform ligament (Fig. 4).
DISCUSSION
We demonstrated that in a typical case of torsion of the lipomatous appendage of the falciform ligament, the findings of serial US and CT may lead to the decision of conservative treatment. The change in echogenicity and echo pattern of the lesion for a relatively short-term period on serial US, and the poor enhancement of the lesion and its close relationship to the falciform ligament in multiplanar reformatted CT scans, confirmed the diagnosis of a benign lesion. Finally, complete resolution of the lesion on further follow-up US strongly supported the rationale for conservative treatment.
Pathologies of the falciform ligament such as cyst, lipoma, or isolated gangrene have rarely been reported previously (1, 2, 3). In our case, a cyst or lipoma of the falciform ligament could easily be differentiated by US or CT. Isolated gangrene of the falciform ligament could also be ruled out in our case due to the absence of peripheral enhancement or adjacent peritoneal infiltration on the CT scan.
Torsion of the lipomatous appendage of the falciform ligament has been reported very rarely (4, 5, 6). To the best of our knowledge, the US and CT findings of this entity were described in only 2 case reports, which showed that real-time US and multiplanar reformatted CT images could play an important role in the accurate diagnosis of this phenomenon (5, 6). Real-time US showed a non-compressible, heterogeneous, mass-like lesion that did not move during respiration. Multiplanar reformatted CT images, especially sagittal images, can help to determine its extraperitoneal nature and demonstrate the relationship between the lesion and the falciform ligament. Coulier et al. (6) suggested that torsion of the lipomatous appendage of the falciform ligament should be considered in the differential diagnosis of intra-abdominal focal fat infarction. This entity can be differentiated from other serious diseases that require surgical treatment by its close relationship with the falciform ligament on CT and real-time US.
Recently, several reports have suggested that omental infarction and torsion of the appendage could successfully be treated conservatively (7, 8). Therefore, as with other intra-abdominal focal fat infarctions, if torsion of the lipomatous appendage of the falciform ligament could be diagnosed accurately, unnecessary operations can be avoided. In the present case, we initially decided to treat conservatively because our patient suffered from acute hepatitis. During conservative treatment, the symptom was gradually relieved and the characteristics of the lesion were changed on serial follow-up US. This implied that the lesion was more likely to be an inflammatory lesion rather than a tumorous condition. Clinical and serial US findings in our patient provided the rationale for conservative treatment.
In conclusion, torsion of lipomatous appendage of the falciform ligament can be diagnosed accurately by real-time US and multiplanar reformatted CT. Clinical and serial US findings such as the relief of symptoms or changes in lesion characteristics can aid in making appropriate decisions for conservative treatment.

 XML Download
XML Download