

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Schwannomas are mostly benign neoplasms arising from the Schwann cells that form the neural sheath. Schwannomas of the gastrointestinal tract are relatively rare and are known to be separate entities from conventional schwannomas which originate in soft tissue or the central nervous system (1). Of all submucosal tumors in the gastrointestinal tract, only 2% to 6% have been reported as schwannomas (2). Most gastrointestinal schwannomas occur in the stomach. Schwannomas in the colon are quite rare. Here, we introduce a case of isolated colonic schwannoma and review the recent literature.
CASE REPORT
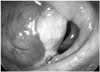
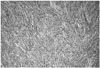
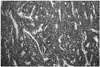
A 79-year-old woman was referred to our colorectal outpatient department for further evaluation and management of an incidentally discovered mass in the ascending colon. She had a medical history of hypertension treated with medication for twenty years. On physical examination, there were no specific findings in her abdomen. Laboratory tests including routine complete blood count, liver function test, and urine analysis were within normal ranges. A colonoscopy was performed and a 4 cm sized intraluminal protruding submucosal tumor, about 70 cm near the anal verge, was found in her ascending colon (Fig. 1). Subsequent biopsy was performed and the pathology showed granulation tissue formation with suppurative inflammation. Multidetector computed tomography (CT) of the abdomen was performed. The pre-contrast image showed a well-defined isodense mass in the ascending colon (Fig. 2A). There was no calcification. On the contrast-enhanced image, the mass showed homogenous enhancement and thin enhancement of intact colonic mucosa was noted (Fig. 2B, C). There were several small perilesional lymph nodes along the ileocolic vessel. The preoperative impression was a submucosal tumor such as neurogenic tumor, leiomyoma, or lymphoma. Her serum carcinoembryonic antigen was 1.4 ng/mL. Our surgeon performed laparoscopic assisted right hemicolectomy with side to side ileocolic anastomosis. Gross examination of the ascending colon revealed a yellowish gray fungating mass measuring 4.1 × 3.4 cm (Fig. 3). On microscopic evaluation, the tumor was composed of plump spindle cells with an occasional fascicular pattern. The tumor cells had normochromatic elongated nuclei without significant nuclear atypia. Mitoses were present in 2/50 high power fields but no atypical forms were identified. Immunohistochemical staining was strongly positive for S-100 protein, but negative for CD34 and CD117 (Figs. 4, 5). The patient was diagnosed with a colonic schwannoma. Thirty-one regional lymph nodes were resected and the pathology revealed reactive hyperplasia. The patient's postoperative course was uneventful and there was no recurrence or metastasis after one year of follow-up.
DISCUSSION
Although the number of reports of gastrointestinal schwannomas has increased with advances in immunohistochemical staining, primary gastrointestinal schwannomas are still rare tumors (2). In the gastrointestinal tract, this tumor mostly occurs in the stomach. Colonic schwannomas are quite rare, comprising 6.1% of gastrointestinal schwannomas reported in previous studies (3). There is no gender predilection in the incidence of colonic schwannomas and they most commonly appear after the sixth decade of life (4). Although usually asymptomatic, colonic schwannomas may cause clinical symptoms such as bleeding, constipation, and anal pain depending on the size and location (2, 5).
Imaging diagnosis of schwannoma before surgery is not easy. According to a previous review of colonic schwannomas in Japan, only 4 of 41 cases (10%) were correctly diagnosed as schwannoma preoperatively (6). Preoperative imaging can be helpful to define the exact tumor location and obtain information about the tumor. However, imaging cannot provide detailed information about benign or malignant features of the tumor and there is overlap in imaging features between schwannomas and other submucosal tumors. On CT, schwannomas usually appear as well defined, round, mural masses with homogeneous enhancement and no evidence of cystic changes, necrosis, hemorrhage or calcification (1). However, small gastrointestinal stromal tumors (GISTs) with low malignant risk may present CT findings similar to schwannomas (1). It has been reported that perilesional lymphadenopathy are more often observed in gastric schwannomas than in gastric GIST (7). Although it is not certain, these lymph nodes are presumed to be reactive hyperplasia due to the fact that gastric schwannomas include many inflammatory cells (7). According to the report, perilesional lymphadenopathy may be helpful for differentiation between gastrointestinal schwannoma and GIST. Primary or secondary lymphomas also have CT findings similar to schwannomas because they show homogenous enhancement before treatment. Accurate preoperative diagnosis of schwannoma is not easy, although the degree of lymph node enlargement can be helpful for differentiating schwannomas from lymphomas because lymphomas are commonly associated with significant lymph node enlargement in the mesentery and retroperitoneum (1). Therefore, preoperative histological examination is usually performed.
Gastrointestinal schwannomas may share gross morphological features with other submucosal tumors. Endoscopic biopsy does not always provide an accurate diagnosis because it is difficult to obtain sufficient biopsy tissue volume in some cases due to tumor hardness (2). In our patient, the result of endoscopic biopsy was granulation tissue formation with suppurative inflammation, which was not helpful for diagnosis. Large forceps biopsy or endoscopic ultrasound-guided biopsy may improve the diagnostic yield (6). For definite diagnosis, immunohistochemistry is usually necessary. Characteristically, schwannomas are composed of spindle cells showing strong positivity for S-100 protein and vimentin, and variable positivity for glial fibrillary acidic protein, while showing negativity for CD34 and CD117. These patterns allow for differentiation of schwannomas from GISTs, gastrointestinal autonomic nerve tumors, and leiomyomas (2, 3).
There are fourteen case reports of colonic schwannomas written in English or Korean and these reports provide accessible information about imaging findings (6, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19). We reviewed these cases as well as ours (Table 1). The mean age of patients was 61.7 years (range, 49-79 years) and the male to female ratio was 1:2. The mean size of tumors was 3.6 ± 2.1 cm. Most of the patients had no symptoms and the tumor was detected on screening colonoscopy. In 6 patients (40%, 6/15), the tumor was located in the ascending colon. Most of the cases showed homogenous enhancement on the preoperative CT. A definite preoperative imaging diagnosis was not made in most cases, but instead, nonspecific submucosal tumor was the most common preoperative diagnosis. Endoscopic biopsy was performed in three patients, but only one patient (16) was accurately diagnosed with schwannoma after multiple colonic biopsies. All the patients underwent surgical resection for treatment.
In general, gastrointestinal schwannomas follow a benign clinical course. Once a schwannoma is diagnosed preoperatively, minimal invasive treatment such as endoscopic resection (2) may be considered instead of aggressive surgery. Therefore, efforts to diagnose schwannomas preoperatively are very meaningful. On CT, homogenous enhancement patterns may be helpful for differentiating schwannomas from other submucosal tumors such as GISTs. Multiple endoscopic biopsies or endoscopic ultrasound-guided biopsy can be very helpful in improving diagnostic yield.
In conclusion, although schwannoma in the colon is a rare type of submucosal tumor, preoperative diagnosis is important for a proper surgical plan. When a colonic submucosal tumor with homogenous enhancement is observed, efforts for preoperative diagnosis such as multiple endoscopic biopsy or ultrasound-guided biopsy should be considered under the radiologic impression of schwannoma.



 XML Download
XML Download