

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The aim of this study was to evaluate the safety and efficacy of SEAL aortic stent-graft for abdominal aortoiliac aneurysms.
Materials and Methods
Between October 2007 and January 2014, 33 patients with abdominal aortoiliac aneurysms were treated with SEAL aortic stent-graft. We evaluated the technical success rate, clinical and CT follow-up periods, major complications, need for additional interventional treatment, aneurysm-related mortality and clinical success rate.
Results
SEAL bifurcated aortic stent-graft was successfully placed in 32 patients (97%). Clinical and CT follow-up periods were 24 and 14 months, respectively. Endoleak developed in 13 patients (41%): spontaneous regression or decrease in 6, need for additional treatment in 4 and follow-up loss in 3. Significant stenosis of stent-graft occurred in 4 patients (12%) and was treated with stenting in 3. Migration of stent-graft was noted in 3 patients (9%) and treated with additional stent-grafting. Aneurysm-related mortality was 9% (3 of 33). The placement of SEAL stent-graft was effective in 26 patients (79%).
Conclusion
The placement of SEAL aortic stent-graft was safe and effective in patients with aneurysms of abdominal aorta and iliac arteries. However, complicating endoleaks, stenosis and migration of the stent-graft developed during the follow-up. Therefore, regular CT follow-up seems to be mandatory.
Figures and Tables

 | Fig. 2A 74-year-old female with abdominal aortic aneurysm (patient number 7 on Table 1).
A. Preimplantation abdominal aortogram demonstrated "hostile" proximal neck (arrow) which has flask shaped appearance.
B. Postimplantation abdominal aortogram showed good placement of aortic stent-graft without evidence of endoleak.
C. Volume-rendering CT image showed no endoleak on 5 days of the placement of aortic stent-graft.
D. Maximum intensity projection CT image revealed newly developed type 3 endoleak (arrow) between main body and right limb stent-graft on 48 months after the placement of aortic stent-graft.
|
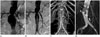
 | Fig. 3An 82-year-old male with abdominal aortic aneurysm with bilateral common iliac artery involvement (patient number 24 on Table 1).
A. Preimplantation abdominal aortogram showed diffuse dilatation of infrarenal abdominal aorta and bilateral common iliac arteries. The proximal neck had "hostile" anatomy due to severe angulation.
B. Postimplantation abdominal aortogram showed good placement of aortic stent-graft without evidence of endoleak. However, left proximal limb stent-graft (arrow) showed significant stenosis due to angulation.
C, D. On 19 days after aortic stent-graft placement, we performed balloon angioplasty (C) and placement of balloon-expandable stent (D) at left proximal limb stent-graft. There was a waist (arrow) during balloon angioplasty showing significant stenosis.
|
Table 1
Summary of 33 Patients with Aortoiliac Aneurysms Treated with SEAL Aortic Stent-Graft Placement

| Pts | Sex/Age | Initial Diagnosis* | Proximal Neck | CIA | EIA | SG Type‡ | TS§ | Endoleak∥ | Other Cx¶ | CS** | Cause of Death | Figures | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Diameter | Length | Angle | Wall† | Diameter | Length | Diameter | Type | Detection Time | Additional Intervention | Outcome | |||||||||
| 1 | M/72 | AAA | 28 | 25 | 35 | T | 18 | 40 | 8 | B | O | Steno | O | Aspiration | |||||
| 2 | M/79 | AAA with R | 26 | 30 | 5 | T | 16 | 28 | 8 | B | O | Steno | O | Sepsis | |||||
| 3 | M/68 | IAA | 28 | 105 | 24 | 55 | 11 | B | O | O | |||||||||
| 4 | M/62 | IAA | 28 | 180 | 19 | 140 | 12 | B | O | O | |||||||||
| 5 | M/64 | AAA | 24 | 35 | 18 | T | 12 | 56 | 6 | B | O | O | |||||||
| 6 | M/56 | AAA | 20 | 35 | 15 | 13 | 68 | 7 | B | O | O | Gastric cancer | |||||||
| 7 | F/74 | AAA | 34 | 0 | 25 | 12 | 39 | 7 | B | O | 3 | N (48 mo) | Additional stent-graft | On F/U | Migr | O | Fig. 2 | ||
| 8 | M/69 | AAA + IAA | 26 | 35 | 60 | 46 | 77 | 8 | B | O | O | ||||||||
| 9 | M/78 | AAA | 19 | 21 | 51 | 16 | 27 | 8 | B | O | O | ||||||||
| 10 | M/66 | AAA | 32 | 16 | 11 | 18 | 32 | 7 | B | O | 1B | N (59 mo) | Additional stent-graft | F/U loss | Migr | X | Delayed AAA rupture | ||
| 11 | M/65 | AAA | 27 | 40 | 18 | C | 15 | 25 | 9 | B | O | 2 (IMA) | R | IMA embolization | Disapp | Steno | O | ||
| 12 | M/75 | AAA | 22 | 50 | 35 | C | 16 | 25 | 10 | B | O | 1B | R | ↓ | O | ||||
| 13 | M/69 | AAA + IAA | 20 | 50 | 13 | 52 | 45 | 12 | B | O | O | ||||||||
| 14 | M/83 | AAA with CR | 32 | 33 | 116 | T | 19 | 33 | 11 | B | X | X | AAA rupture | ||||||
| 15 | F/76 | AAA | 32 | 30 | 39 | 24 | 24 | 8 | B | O | O | ||||||||
| 16 | F/88 | AAA | 23 | 79 | 89 | 17 | 33 | 8 | B | O | 1A | R | F/U loss | X | |||||
| 17 | M/81 | AAA | 31 | 30 | 57 | C | 21 | 35 | 9 | B | O | 1B | R | F/U loss | X | ||||
| 18 | M/67 | AAA with R | 26 | 45 | 32 | 14 | 25 | 7 | B | O | 1B | N (41 mo) | Additional stent-graft | On F/U | Migr | O | |||
| 19 | M/64 | AAA | 26 | 55 | 44 | T | 13 | 40 | 7 | B | O | O | |||||||
| 20 | M/70 | AAA + IAA | 20 | 75 | 46 | 39 | 40 | 10 | B | O | 2 (L) | R | ↓ | Steno | O | ||||
| 21 | F/77 | AAA with R | 20 | 27 | 91 | 12 | 18 | 9 | B | O | O | ||||||||
| 22 | F/75 | AAA with CR | 23 | 45 | 41 | T | 14 | 20 | 7 | B | O | O | |||||||
| 23 | M/58 | AAA with CR | 23 | 36 | 33 | 16 | 37 | 10 | B | O | O | ||||||||
| 24 | M/82 | AAA | 22 | 27 | 68 | T | 17 | 39 | 11 | B | O | 2 (IMA) | R | F/U loss | X | Acute MI | Fig. 3 | ||
| 25 | F/85 | AAA with R | 17 | 30 | 30 | C | 9 | 20 | 6 | B | O | X | AAA rupture | ||||||
| 26 | M/71 | AAA | 21 | 75 | 30 | 12 | 20 | 11 | B | O | 2 (IMA) | R | ↓ | O | |||||
| 27 | M/74 | AAA | 33 | 59 | 93 | T | 24 | 36 | 11 | B | O | 2 (L) | R | Disapp | X | ||||
| 5 | N (28 mo) | On F/U | |||||||||||||||||
| 28 | M/80 | AAA | 26 | 35 | 89 | 25 | 25 | 11 | B | O | 2 (L) | R | ↓ | O | |||||
| 29 | M/80 | AAA | 25 | 24 | 78 | 15 | 39 | 9 | B | O | O | ||||||||
| 30 | M/66 | AAA | 22 | 21 | 74 | 12 | 21 | 10 | B | O | O | ||||||||
| 31 | M/84 | AAA | 28 | 35 | 62 | 20 | 20 | 9 | B | O | O | Medullary paralysis | |||||||
| 32 | M/76 | IAA with R | 29 | 120 | C | 36 | 55 | 12 | B | O | 2 (IIA) | R | ↓ | O | |||||
| 33 | M/79 | AAA | 25 | 30 | 38 | 20 | 30 | 8 | B | O | O | ||||||||
Note.-*Initial diagnosis: AAA = abdominal aortic aneurysm, IAA = iliac artery aneurysm, R = rupture, CR = contained rupture
†Proximal neck wall: T = thrombosis, C = calcification
‡Stent-graft types: B = bifurcated type, T = tubular type
§Technical success: O = success, X = failed
∥Endoleak type: IMA = inferior mesenteric artery, L = lumbar artery, Endoleak detection time = interval between initial intervention and initially detected time (months), N = newly appeared endoleak, R = residual endoleak, Outcome: F/U = follow-up, Disapp = disappeared endoleak on follow-up CT, ↓ = decreased endoleak on follow-up CT
¶Other complications: Steno = limb stent-graft stenosis, Migr = stent-graft migration
**Clinical success: O = success, X = failed
![]()
References
1. Brewster DC, Jones JE, Chung TK, Lamuraglia GM, Kwolek CJ, Watkins MT, et al. Long-term outcomes after endovascular abdominal aortic aneurysm repair: the first decade. Ann Surg. 2006; 244:426–438.
2. Lee DY, Kang SG, Choi D, Lee GH, Maeda M, Roh BS, et al. Percutaneous modular stent-grafts in the treatment of abdominal aortic aneurysms. J Endovasc Ther. 2003; 10:752–759.
3. You JH, Park HK, Park CB. Endovascular repair of bilateral iliac artery aneurysm with branched iliac stents: case report and review of the current literature. J Korean Surg Soc. 2013; 85:145–148.
4. Chaikof EL, Fillinger MF, Matsumura JS, Rutherford RB, White GH, Blankensteijn JD, et al. Identifying and grading factors that modify the outcome of endovascular aortic aneurysm repair. J Vasc Surg. 2002; 35:1061–1066.
5. Veith FJ, Baum RA, Ohki T, Amor M, Adiseshiah M, Blankensteijn JD, et al. Nature and significance of endoleaks and endotension: summary of opinions expressed at an international conference. J Vasc Surg. 2002; 35:1029–1035.
6. White GH, Yu W, May J. Endoleak--a proposed new terminology to describe incomplete aneurysm exclusion by an endoluminal graft. J Endovasc Surg. 1996; 3:124–125.
7. White GH, May J, Waugh RC, Chaufour X, Yu W. Type III and type IV endoleak: toward a complete definition of blood flow in the sac after endoluminal AAA repair. J Endovasc Surg. 1998; 5:305–309.
8. Katsargyris A, Botos B, Oikonomou K, Pedraza de Leistl M, Ritter W, Verhoeven EL. The new C3 Gore Excluder stent-graft: single-center experience with 100 patients. Eur J Vasc Endovasc Surg. 2014; 47:342–348.
9. Iwakoshi S, Ichihashi S, Higashiura W, Itoh H, Sakaguchi S, Tabayashi N, et al. A decade of outcomes and predictors of sac enlargement after endovascular abdominal aortic aneurysm repair using zenith endografts in a Japanese population. J Vasc Interv Radiol. 2014; 25:694–701.
 XML Download
XML Download