

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Vertebral artery loop formation (VALF) is an anatomic variation that possibly causes cervical nerve root compression. Clear visualization of the neural foramen (NF) is essential for pain intervention and seems to be more important if the cause of NF stenosis is VALF. Pain intervention doctors routinely use MR images to investigate pathological changes in the spine and to plan their treatment approach. Moreover, pain intervention doctors performing cervical injections, such as selective transforaminal epidural block (STEB), are familiar and find it easy to work with oblique sagittal MR images as they are similar to the fluoroscopic en face images routinely used by intervention doctors in these procedures. Conventional sagittal MR images do not provide a clear view of the NF and are limited in their ability to evaluate abnormalities in the NF because of the nearly 45-degree oblique course of the NF with regard to the sagittal plane. We report a case of VALF clearly depicted on oblique sagittal MRI.
CASE REPORT
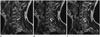
A 50-year-old woman visited the hospital with pain in both upper extremities, and especially complained of moderate to severe pain in the left shoulder area since the past one month. The visual analogue scale was 6. A cervical spine MRI was performed using a 1.5-T MR scanner (GE Medical Systems; Signa HDxt; USA). Fig. 1 shows the scout conventional sagittal and oblique sagittal MR images through the NF. MR images showed a signal-void structure in the left C5-6 NF compressing the left C6 nerve root (Fig. 2). Conventional sagittal MR images did not clearly depict the NF abnormality (Fig. 2B) and the differentiation between herniated disc and vascular anomaly such as VALF was not clear. Oblique sagittal MR images (Fig. 3) definitively showed that the abnormality of the left C5-6 NF was VALF. There were several treatment approaches available, and among them, STEB was the most effective treatment option. Pain intervention doctor decided to perform a series of single epidural block (SEB) via the posterior and paramedian approach at the C7-T1 level during regular follow-up at the outpatient department although SEB was less effective but a safer treatment option than STEB. The patient reported that her pain was markedly relieved after several sessions of SEB with persistence of only mild pain.
DISCUSSION
VALF was first reported in a cadaveric study (1), and the reported incidence of VALF was 7.51% in a clinical study of patients with cervicobrachial pain (2). Incorrect diagnosis of VALF as disc herniation may lead to a possible injury to the vertebral artery during pain intervention such as STEB. Furman et al. (3) reported intravascular needle placement in 19.4% of 504 fluoroscopically-guided cervical selective nerve root block procedures. Unawareness of inadvertent needle injury to the vertebral artery during the procedure can lead to a fatal outcome ranging from dissection, thrombosis, to brainstem hemorrhagic infarction. This is the situation in case of the vertebral artery having a normal course and the risk of vertebral artery injury is significantly increased if there is a vascular anomaly such as VALF. Therefore, optimal visualization of the NF abnormality of the cervical spine is very important for pain intervention doctors. Kim et al. (4) reported a case of VALF depicted on conventional sagittal MR imaging, but the NF abnormality was not clearly depicted. Oblique sagittal MR imaging using 45 degree cuts through the NF depicts the abnormalities en face and may delineate the lesion better (5). It aids pain intervention doctors in understanding the structures in the cervical NF because they are familiar with the fluoroscopic en face images. Therefore, oblique sagittal MR images can reduce the risk of unexpected vertebral artery injury. A review of the literature indicates that cervical levels involved with VALF that produce symptoms are frequently observed at C4-5 and C5-6 (4). The left vertebral artery is involved more often than the right vertebral artery. Rarely, bilateral or multilevel VALF occurs (4).
We have described the case of a 50-year-old female with VALF that was clearly depicted on oblique sagittal MRI.


 XML Download
XML Download