

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The serratus anterior is a flattened sheet of muscle originating from the first through the ninth ribs and inserting along the medial border of the costal surface of scapula. The function of serratus anterior is to protract and rotate the scapula, thus providing a full range of motion at glenohumeral joint. It also keeps the scapula closely opposed to the thoracic wall (1, 2).
Only a few cases of isolated aplasia of the serratus anterior muscle have been reported (2, 3). Usually, it presents as a part of the combination of shoulder girdle muscle anomalies (4, 5, 6). Here, we report a case of a 30-year-old male with unilateral complete aplasia of the right serratus anterior muscle and winging of the right scapula, which was incidentally found through chest radiography and CT scan. This unusual case emphasizes the importance of paying careful attention to chest wall structures while interpreting a plain radiography.
CASE REPORT
A 30-year-old Korean male presented with left flank pain. He complained of tenderness on his left ribs and left scapula areas, and showed decreased range of motion in the left shoulder. He described having more pain when he took left-side down lateral decubitus. There was tenderness, rated 6 to 7 on the numerical rating scale, of the area. He had a 1 month history of strenuous physical activities.
His medical history was not significant. He had never been hospitalized or operated on before. His family history was nonspecific and there was no known congenital disorder. He had smoked for fifteen pack-years and socially drunk alcohol. The patient's review of systems was unremarkable.
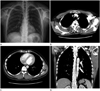
A chest radiograph showed noted absence of right serratus anterior muscle. The lateral chest wall shadow normally is composed of serratus anterior muscle, intermuscular fat plane, latissimusdorsi muscle, and subcutaneous fat from medial to lateral. But the patient's chest radiograph didn't show shadows of the right serratus anterior muscle or the intermuscular fat plane, and it showed the right scapula elevated by 0.9 cm and its inferior pole medially rotated (Fig. 1A). A subsequent chest CT scan showed an increased distance between the medial border of right scapula and the rib cage compared to the opposite side, which is compatible with medial winging of right scapula (Fig. 1B). Although the other muscles contributing to the shoulder girdle were normal, the CT scan showed an absence of the right serratus anterior muscle (Fig. 1C, D). There was no remarkable difference in the size and shape of the two scapulae.
After conservative treatment, the left flank pain was relieved. Because the patient didn't complain of any symptoms on his right shoulder, no treatment about his was performed on his right shoulder.
DISCUSSION
Scapular winging is a rare debilitating condition that limits the function of the upper extremity (1), and it can be subdivided into medial and lateral according to the direction of the rotation of the scapula.
Medial winging of the scapula is caused by an abnormality of the serratus anterior muscle. The serratus anterior is solely innervated by a long thoracic nerve, originating from the anterior rami of the fifth through seventh nerves (1). Most of the cases of medial winging of the scapula have been associated with neurologic causes from the injury of the long thoracic nerve (1). The medial scapular winging caused by isolated aplasia of the serratus anterior muscle is extremely rare (2, 3).
The most common congenital abnormality involving shoulder girdle is Sprengel deformity (2), which consists of congenital high scapula and limited motion of the shoulder, often includes the regional muscle hypoplasia (7, 8). The most commonly affected muscles are the trapezius, the pectoralis major, and the sternocleidomastoid muscles. Other muscles such as the serratus anterior, the levator scapulae, the infraspinatus, latissimusdorsi, the teres major, the pectoralis minor, and the rhomboids are less affected (2). Sprengel deformity is almost always associated with other malformations of cervicothoracic vertebrae or thoracic rib cage (9). In Sprengel deformity, congenital elevation of the scapula is caused by an interrupted caudal migration of the scapula and is associated with arrested growths of bone and muscle (2, 8, 9).
Poland syndrome is another congenital abnormality involving shoulder girdle. It is characterized by partial or complete aplasia of the pectoralis major muscle (6). Poland syndrome is often accompanied by serratus anterior aplasia and scapular hypoplasia (2).
Chernev and Pessina (2) suggested a new category of deformity composed of serratus anterior muscle aplasia and winged, high-riding, and hypoplastic scapula. They thought this deformity may become a new variant of known congenital syndromes affecting the scapula, such as Sprengel deformity or Poland syndrome.
This case shows isolated absence of serratus anterior and winging and medial rotation of the scapula. These features are compatible with the new disease category that Chernev suggested; but this case is different in the following aspects. First, the degree of high scapula was subtle. This case shows only 0.9 cm elevation of the scapula, contrary to 2-7 cm elevation in the usual cases (8). Secondly, there was no remarkable scapula hypoplasia. Therefore, we can reasonably assume that this case could be a new type of deformity or a mild variant of the deformity that Chernev suggested.
This case is also unique in the course of diagnosis. The previous cases of isolated aplasia of the serratus anterior muscles were diagnosed by either physical exam alone or by physical exam and magnetic resonance imaging. But this case is the first where it was diagnosed incidentally, while examining the chest radiography. The role of the radiologist was important in diagnosing this anomaly. When the shadow of the serratus anterior muscle and the medial rotation of the inferior pole of scapula are not present on the chest radiograph, it can be reasonably assumed that there is aplasia or hypoplasia of the serratus anterior and winging of scapula. While interpreting chest radiograph, the awareness of the characteristic finding of this rare deformity can lead to correct diagnosis of this clinically vague deformity. It can also help make an early diagnosis of the cause of winged scapula and reduce unnecessary examinations. This case shows us the importance of thorough reading with high index of suspicion for abnormalities, when interpreting chest radiographs in everyday practice.
 XML Download
XML Download