

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The ophthalmic artery (OA) is the first major branch of the ophthalmic segment of the internal carotid artery (ICA). In the majority of cases, the OA arises from the anteromedial or superomedial aspect of the ICA, and it is extremely rare that the OA arises from the medial or posteromedial aspect of the ICA. Although rare, the middle meningeal artery, the anterior cerebral artery, the basilar artery, and the ICA bifurcation have been observed as variations of the OA's origin (1). A precise understanding of neuroanatomic variations is important in the diagnosis and treatment of vascular lesions in the brain. We suggest that normal variation of origins may be the result of abnormal development of the primitive OA.
CASE REPORT
Case 1
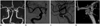
A 55-year-old female patient was hospitalized with a 10-day history of left facial palsy and weakness in her left upper extremity. The patient had been treated for hypertension. She had no history of head trauma and there were no significant abnormal findings, except for slight elevation of erythrocyte sedimentation rate level seen in the bloodwork. Upon admission, a brain magnetic resonance imaging (MRI) was done and showed a chronic lacunar infarction at the right thalamus, a resolved hematoma at the left basal ganglia, and diffuse microbleeds. Magnetic resonance angiography (MRA) revealed a bulging lesion at the posteromedial aspect of the ophthalmic segment of the right ICA that was suspected to be an aneurysm (Fig. 1A). There was a small vessel at the medial side of the bulging lesion, which raised the possibility of an infundibular dilatation but we could not find the continuity between the small vessel and the bulging lesion. To confirm the lesion, digital subtraction angiography (DSA) with three-dimensional (3D) rotational angiography (RA) was performed and we found the infundibular dilatation originated from the posteromedial aspect of the ophthalmic segment of the right ICA. There was a vessel arising from the medial apex of the infundibular dilatation and running forward. We regarded the vessel as the OA considering the direction of the distal part of the vessel and correlation with the eye. The lesion suspected to be an aneurysm based on the brain MRA was confirmed to be an infundibular dilatation at the origin of the OA (Fig. 1B-D). The patient's symptoms improved with conservative treatment and the patient was discharged without any other procedure or further evaluation.
Case 2
A 58-year-old female patient was hospitalized with complaints of a headache and forehead numbness. The headaches began about 10 years ago and have persisted. Eighteen months ago, a brain MRI showed no abnormal findings and the patient underwent conservative treatment. However, the symptom returned a month ago and aggravated. The patient was treated for hypertension and diabetes. Her mental state was normal. The motor and sensory system examination were also normal in her both upper and lower extremities and were no significant abnormal findings were seen in the bloodwork. A brain MRA was performed upon admission, and a small bulging lesion was suspected at the medial side of the ophthalmic segment of the right ICA (Fig. 2A). DSA with 3D RA was performed to obtain an accurate diagnosis. Angiography showed an aneurysm from the medial side of the ophthalmic segment of the right ICA (Fig. 2B). The 3D-reconstruction of the lesion clearly revealed a small aneurysm with an aneurysmal neck at the carotid-ophthalmic junction (Fig. 2C, D). The OA arises from the wall of the aneurysm and runs forward. The small lesion suspected to be aneurysm at brain MRA was confirmed as a cerebral aneurysm formed at the carotid-ophthalmic junction. Since the aneurysm was very small and the OA arose from the aneurysm, the patient did not undergo any other procedure or further evaluation and was discharged.
DISCUSSION
Embryogenesis of the OA is very complex. Vascularization of the optic cup is derived from two branches of the primitive ICA called the primitive ventral ophthalmic arteries (VOA) and dorsal ophthalmic arteries (DOA). According to Lasjaunias et al. (2), the VOA originates from the anterior cerebral artery and passes through the optic canal while the DOA originates from the ICA (Fig. 3A). Then, two anastomoses are formed, one near the optic nerve in the orbit between the VOA and DOA, and one between the VOA and the ICA (Fig. 3B, C). The proximal parts of the VOA and DOA regress, resulting in the formation of the primitive OA (Fig. 3D). According to Padget (3), the DOA first appears at the opposite side of the bifurcation of the primitive ICA (Fig. 4A). The DOA then moves proximally to form an anastomosis with the VOA, resulting in the formation of the primitive OA (Fig. 4B-D). The proximal migration of the DOA is called "caudal migration".
To the best of our knowledge, the OA usually arises from the anteromedial surface of the ICA. Regarding the course of the OA, it originated from the ICA and first ran medially and then turned laterally on the upper surface of the optic strut and below the intracranial optic nerve. In a study of 58 cadavers (4), 53.6% of the OA arises from the anteromedial aspect of the ICA, 37.5% from the superomedial aspect, 7.1% from the medial aspect, and 1.8% from the anterosuperior aspect. Gibo et al. (5) reported that 78% of the time, the OA originates from the medial third of superior surface of the ICA, 22% from central third, and none from lateral third. In both of our cases, the OA arises from the medial and posteromedial aspect of the ICA. We suppose that the atypical origin of the OA can be explained by the OA embryogenesis. It is likely that an abnormal anastomoses between VOA and ICA may occur in development period. It could have also happened during the process called "caudal migration".
By understanding embryogenesis, we can also explain the reason why infundibular dilatation or aneurysm is found at an unusual sites as origin of the OA. Baltsavias et al. (6) reported on an aneurysm of the ICA accompanied with the persistent ventral ophthalmic artery, and Tanaka (7) reported on an aneurysm of the ICA accompanied with the persistent DOA. We suggest if the proximal parts of the VOA partially regress or fail to regress, a remnant of the VOA can remain. It is possible that the remnant parts may presented as an infundibular dilatation or aneurysm.
It is important to differentiate an infundibular dilatation or aneurysm from other paraclinoid aneurysms on angiography. By confirming the precise location of origin of the OA and aneurysmal sac formed at the carotid-ophthalmic junction, we can rule out other paraclinoid aneurysms. However, the incidence of carotid-ophthalmic aneurysms are low. In the first cooperative study of 2695 intracranial aneurysms, only 5.4% were carotid-ophthalmic aneurysms (8). We can also define the infundibular dilatation as the OA's site of origin by several typical findings. The infundibular dilatation is round or conical in shape, a maximum diameter of less than 3 mm, without an aneurysmal neck, and with an artery arising from its apex. The incidence of infundibular dilatation detected by angiography or at autopsy ranges from 7% to 25%, and increases with age (9). Infundibular dilatation most often affects the origin of the posterior communicating artery at its junction of the ICA, but and infundibular dilatation affecting the origin of the OA at its junction has not been reported before.
The complex embryogenesis of the OA and normal variation should be further evaluated. Although the OA originating from the medial or posteromedial aspect of the ICA is extremely rare, awareness of rare variations in anatomic structures is important for the diagnosis and treatment of vascular lesions. In addition, the MRA findings of the infundibular dilatation at unusual sites of origin of the OA can be misdiagnosed as an aneurysm. We recommend performing a DSA along with a 3D RA since it can provide useful information in confirming the anatomy of the ophthalmic artery and the presence of an aneurysm.



 XML Download
XML Download