

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tendinous xanthoma is commonly seen in patients with familial hypercholesterolemia (FH) and produces nodular masses in the Achilles tendon and other tendons, and earlier clinical diagnosis of FH depends on the detection of xanthomas (1). Early detection of FH is important in order to alter its clinical course (2). To our knowledge, the sonographic findings of tendinous xanthoma in the multiple tendons have been rarely reported. We present a case of multiple xanthomas of ankles and elbows in a patient with FH.
CASE REPORT
A 52-year-old woman was referred for evaluation of multiple soft tissue lesions. She first noticed lesions of the bilateral Achilles tendons at the age of 30. Subsequently, similar lesions that were slightly painful gradually developed in the elbows and feet. The laboratory studies showed slightly increased levels of total cholesterol (230 mg/dL, upper normal value 200 mg/dL) and low-density lipoprotein (LDL) (146 mg/dL, upper normal value 130 mg/dL). She also had family history of similar lesions. Radiographs, sonography, and MR studies were performed for the selected lesions.
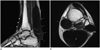
Radiographs of the ankles and elbows revealed normal osseous architecture with increased soft tissue density posterior to the ankle and elbow joints along the expected course of the Achilles and triceps tendon (Fig. 1). Sonography demonstrated marked enlargement and mixed echoic pattern in the bilateral Achilles tendons, and similar findings were also shown in the triceps, anterior tibialis, posterior tibialis, peroneus longus, and flexor hallucis longus tendons (Figs. 2, 3). MR imaging of the ankles showed marked heterogeneous fusiform enlargement of the above multiple tendons with regions of increased signal intensity and numerous interspersed trabeculated linear areas with diminished signal intensity (Fig. 4).
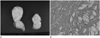
The patient underwent open biopsy of the triceps tendon lesion. Histopathology showed numerous lipid-filled foamy cells consistent with tendinous xanthoma (Fig. 5).
DISCUSSION
FH is characterized by an elevated serum LDL concentration. Due to decreased numbers of functionally active LDL receptors, the metabolism and elimination of LDL are impaired and cholesterol is subsequently accumulated in soft tissues. This leads to the development of xanthoma in the Achilles and other tendons and accelerated development of coronary artery disease (1). Coronary heart disease rarely occurs before the development of tendon xanthoma (2). So, early detection of tendinous xanthoma can protect patients with FH from cardiovascular atherosclerosis and early death.
Tendinous xanthomas are grayish-yellow to yellow masses composed of lipid-filled xanthoma cells, extracellular cholesterol, and inflammatory cells. On clinical examination, these deposits cannot be separated from the underlying tendon, and they move with the tendon on flexion and extension. The enlargement is fusiform or nodular and is usually non-tender and bilateral (3, 4). The most common locations are the extensor tendons of the hands, the feet, and the Achilles tendons. The average age of onset of Achilles tendon xanthoma is 22, but onset during childhood occurs in homozygous patients and is associated with more severe coronary atherosclerosis (5).
Radiographs of tendinous xanthomas show soft tissue enlargement of uniformly increased density and absence of calcifications. At the ankle, symmetric bilateral fusiform soft tissue enlargement of the Achilles tendon suggest the diagnosis of tendon xanthomas (5, 6).
Ultrasonography (US) with high resolution linear-array equipment has been rated as superior to MRI, for the evaluation of xanthomatous lesions (7). Sonography shows marked enlargement and mixed echoic pattern of the affected tendons. Descamps et al. (8) reported that Achilles tendon of thickness above 5.8 mm was the most useful threshold for the diagnosis of FH, procuring sensitivity of 75% and specificity of 85%. In our case, Achilles tendon thickness was measured to be 30 mm on US, and this was notable not only for the pronounced enlargement of the Achilles tendon, but also for its similar findings at the triceps, anterior tibialis, posterior tibialis, peroneus longus, and flexor hallucis longus tendons.
Our case shows the typical findings of fusiform tendon enlargement, consisting of globular heterogeneous signal intensity on T1- and T2-weighted sequences and interspersed trabeculated areas of diminished signal intensity coursing throughout the affected areas. These characteristic of low-signal trabeculations represent areas of residual normal collagen fascicles; the globular areas of mixed signal intensity represent the xanthomatous deposits (9). Not only bilateral Achilles tendons, but also other multifocal tendons were involved in our case.
In conclusion, multiple tendon xanthomas are pathognomic for the familial hypercholesterolemia, so the role of radiologist is important for early diagnosis that can alter its clinical course. Imaging findings are typical; symmetric bilateral fusiform soft tissue enlargement of the Achilles tendon and similar findings of other multifocal tendons should suggest the diagnosis of tendon xanthoma in familial hypercholesterolemia.



 XML Download
XML Download