

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
We evaluated the CT findings of pulmonary thromboembolism (PTE) in patients with malignancy and compared these findings with the control group who had PTE without malignancy.
Materials and Methods
During the last 5 years, 490 patients had PTE on CT examination. We classified the patients into two groups based on the presence and absence of malignancy. Among the included participants, 155 patients had malignancy and 335 patients did not have malignancy. The clinical and laboratory findings were reviewed. We analysed the CT findings for the level of the involved vessel, pulmonary embolism (PE) index, and association with deep vein thrombosis (DVT) on the leg. Differences were reviewed retrospectively. The most common primary malignancy was in the lung.
Results
In the group with malignancy (155), 50 patient (32.3%) presented symptoms for PTE. The level of involved vessels were the main (15, 9.7%), below lobar (91, 58.7%), and below segmental (49, 31.6%). The PE index was 18.1 ± 14.75, and 27 patients (42.2%) had DVT. In the control group (335), 216 patients (64.5%) presented symptoms for PTE. The level of the involved vessels were the main (75, 22.4%), below lobar (163, 48.6%), and below segmental (97, 29%). The PE index was 23.55 ± 18.025, and 98 patient (41.4%) had DVT. The comparisons of the findings showed significant differences (p = 0.01) except for DVT.
Figures and Tables
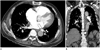 | Fig. 1A seventy five years old man with cholangiocarcinoma and multiple metastasis. He had no symptom related with pulmonary thromboembolism. The axial contrast CT images at the level of left atrium (A) and coronal reconstructed image (B) shows thrombus in both lower segmental arteries (arrows). Pulmonary embolism index is 5 and deep vein thrombosis was not present.
|

References
1. Wildberger JE, Mahnken AH, Das M, Küttner A, Lell M, Günther RW. CT imaging in acute pulmonary embolism: diagnostic strategies. Eur Radiol. 2005; 15:919–929.
2. Kucher N, Goldhaber SZ. Management of massive pulmonary embolism. Circulation. 2005; 112:e28–e32.
3. Heit JA, O'Fallon WM, Petterson TM, Lohse CM, Silverstein MD, Mohr DN, et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study. Arch Intern Med. 2002; 162:1245–1248.
4. Kirwan CC, Nath E, Byrne GJ, McCollum CN. Prophylaxis for venous thromboembolism during treatment for cancer: questionnaire survey. BMJ. 2003; 327:597–598.
5. Prandoni P, Lensing AW, Cogo A, Cuppini S, Villalta S, Carta M, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med. 1996; 125:1–7.
6. Sørensen HT, Mellemkjaer L, Olsen JH, Baron JA. Prognosis of cancers associated with venous thromboembolism. N Engl J Med. 2000; 343:1846–1850.
7. Douma RA, Kok MG, Verberne LM, Kamphuisen PW, Büller HR. Incidental venous thromboembolism in cancer patients: prevalence and consequence. Thromb Res. 2010; 125:e306–e309.
8. Dentali F, Ageno W, Becattini C, Galli L, Gianni M, Riva N, et al. Prevalence and clinical history of incidental, asymptomatic pulmonary embolism: a meta-analysis. Thromb Res. 2010; 125:518–522.
9. Levitan N, Dowlati A, Remick SC, Tahsildar HI, Sivinski LD, Beyth R, et al. Rates of initial and recurrent thromboembolic disease among patients with malignancy versus those without malignancy. Risk analysis using Medicare claims data. Medicine (Baltimore). 1999; 78:285–291.
10. Qanadli SD, El Hajjam M, Vieillard-Baron A, Joseph T, Mesurolle B, Oliva VL, et al. New CT index to quantify arterial obstruction in pulmonary embolism: comparison with angiographic index and echocardiography. AJR Am J Roentgenol. 2001; 176:1415–1420.
11. Çobanoğlu U. Pulmonary Embolism. In : Çobanoğlu U, editor. Risk Factor for Pulmonary Embolism. Croatia: InTech;2012. p. 1–18.
12. Winston CB, Wechsler RJ, Salazar AM, Kurtz AB, Spirn PW. Incidental pulmonary emboli detected at helical CT: effect on patient care. Radiology. 1996; 201:23–27.
13. Gosselin MV, Rubin GD, Leung AN, Huang J, Rizk NW. Unsuspected pulmonary embolism: prospective detection on routine helical CT scans. Radiology. 1998; 208:209–215.
14. Gladish GW, Choe DH, Marom EM, Sabloff BS, Broemeling LD, Munden RF. Incidental pulmonary emboli in oncology patients: prevalence, CT evaluation, and natural history. Radiology. 2006; 240:246–255.
15. Shinagare AB, Okajima Y, Oxnard GR, Dipiro PJ, Johnson BE, Hatabu H, et al. Unsuspected pulmonary embolism in lung cancer patients: comparison of clinical characteristics and outcome with suspected pulmonary embolism. Lung Cancer. 2012; 78:161–166.
16. Shinagare AB, Guo M, Hatabu H, Krajewski KM, Andriole K, Van den Abbeele AD, et al. Incidence of pulmonary embolism in oncologic outpatients at a tertiary cancer center. Cancer. 2011; 117:3860–3866.
17. den Exter PL, Hooijer J, Dekkers OM, Huisman MV. Risk of recurrent venous thromboembolism and mortality in patients with cancer incidentally diagnosed with pulmonary embolism: a comparison with symptomatic patients. J Clin Oncol. 2011; 29:2405–2409.
18. Palla A, Rossi G, Falaschi F, Marconi L, Pistolesi M, Prandoni P. Is incidentally detected pulmonary embolism in cancer patients less severe? A case-control study. Cancer Invest. 2012; 30:131–134.
 XML Download
XML Download