

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Approximately 1-5% of the spinal schwannomas arise in the sacrum and frequently grow to a considerable size before becoming symptomatic; hence, the term "giant sacral schwannoma" refers to tumors extending into the vertebral body and the extraspinal space (1). Most schwannomas are solid or heterogeneous solid tumors, but they can rarely undergo cystic degeneration, xanthomatous change, or hemorrhage (2). A completely cystic appearance with only thin peripheral wall enhancement is extremely rare.
A few cases of solitary cystic schwannomas arising from the spine have been previously reported (3, 4, 5, 6, 7, 8). To the best of our knowledge, there is only one previous reported case of a giant solitary cystic schwannoma of the sacrum. Here, we describe a rare case of a totally cystic giant sacral schwannoma presenting as lumbar back pain. Institutional review board approval was obtained.
CASE REPORT
A 69-year-old man presented with chronic lower lumbar back pain radiating to the lower limb. The back pain had progressed for 6 months, and the patient did not have any prior neurological symptoms or any history of trauma or surgery.
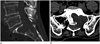
The computed tomography (CT) imaging showed a large osteolytic mass involving the upper sacrum (Fig. 1). The mass was 5.6 × 5.4 × 4.5 cm in size, and marginal sclerosis was noted. The magnetic resonance imaging (MRI) revealed a well-defined unilocular cystic mass in the sacrum, which was occupying most of the left upper sacrum. It partially extended to the retroperitoneum (Fig. 2A-D). The fluid-fluid level with intermediate signal intensity on T1- and T2-weighted images indicated a recent hemorrhage or cystic degeneration of the mass (Fig. 2A, D). The contrast-enhanced T1-weighted images showed thin rim enhancement of the mass, but there was no septum or nodular enhancing in the solid portion (Fig. 2E). The preoperative differential diagnosis were cystic spinal lesions including dermoid cysts, epidermoid cysts, arachnoid cysts, neurenteric cysts, cystic teratomas, meningoceles, primary bone cysts or cystic tumors, and perineural cysts.
The tumor was excised using a posterior midline approach. In the operative fields, the large cystic tumor was associated with the extensive bony erosion involving the sacral body and was found to be firmly attached to the left S1 nerve root. The cystic component of the tumor was aspirated, and this was followed by tumor excision. There were no complications during the postoperative course, and the patient subsequently became free of symptoms.
The histopathologic examination showed a predominantly cystic component with extensive degeneration and hemorrhage (Fig. 3A). Within the few solid components of the tumor, wavy spindle cells with an interlacing, fascicular pattern were observed, whereas in other areas, palisading nuclei in whorled formations and arrangement in rows of eosinophilic processes (Verocay bodies) were noted. The solid components presented two distinct types of tissue patterns; Antoni A is where the spindle cells are arranged in a relatively compact palisading pattern, and Antoni B is comprised of loose reticular, often in cystic arrangements (Fig. 3B). The widespread areas of hemorrhagic, cystic, and microcystic degeneration were noted, but these lacked features of degenerative nuclear pleomorphic changes indicative of ancient schwannoma.
On postoperative day 21, the patient was doing well with no complaints, although the follow-up MRI scan has not been performed.
DISCUSSION
Schwannomas are benign tumors that originate from Schwann cells in the myelinated nerve sheath. The sacral region is an uncommon site for spinal schwannoma, compared to the thoracic or lumbar region (3, 5, 8).
These tumors are generally slow in growth, with common symptoms such as pain or paresthesia developing well before spreading into the extraspinal tissues. However, these tumors sometimes present as huge masses extending into the vertebral body and extraspinal tissues, and then, they are referred to as the giant invasive spinal schwannomas (5, 6, 9, 10). Although the term giant schwannoma is not clearly defined yet, the generally accepted definition is a tumor extending to more than 2 vertebral bodies while eroding the vertebral bodies and extending into myofascial planes, with the extraspinal extension of more than 2.5 cm (9). The giant spinal schwannoma is rare, especially in the sacral region. On the basis of the anatomic location, a giant sacral schwannoma can be classified into 3 types. Each type shows different clinical features as follows: 1) retroperitoneal tumors usually do not have specific symptoms; 2) intrasacral (osseous) tumors present with mild local pain, and neurological deficit is unusual; and 3) spinal tumors (dumb-bell tumors) are usually associated with neurological deficit or other symptoms (7).
MRI is a valuable method for the diagnosis and characterization of the tumor, with regard to size, location, and relations to other organs. The depiction of the tumor originating from an adjacent nerve root is known to be a pathognomonic MRI finding of a neurogenic tumor. On MRI, the typical features of a schwannoma are as follows: T1-weighted images show iso- to hypointense signal intensity compared to the spinal cord, T2-weighted images show hyperintense signal intensity or heterogeneous signal intensity, and contrast enhanced T1-weighted images show good enhancement. The heterogeneous signal intensities on T2-weighted or contrast-enhanced T1-weighted images indicate heterogeneous cellularity and degenerative changes such as necrosis, cyst formation, hemorrhage, fibrosis, and calcification (3, 4, 5, 6, 7, 10). The features of typical spinal schwannomas and giant spinal schwannomas on MRI scans are not significantly different. However, the giant schwannomas show a tendency towards more heterogeneity than the typical tumors (10).
The cyst formation is not an unusual finding, especially in large schwannomas, but this is most often partial and does not involve the entire lesion. The mechanism of cyst formation can be explained by 2 theories. First, the degeneration of the Antoni B cells could lead to cyst formation, which progresses in size over time. Second, tumor growth results in ischemic necrosis. A fluid separation occurs, based on viscosity, protein content, or even hemorrhage, leading to the fluid-fluid levels (6, 8). The nearly complete or complete cystic formation of the spinal schwannomas is rare. A few cases of giant schwannoma with complete cystic change have been reported, and most of these cases involved septation or a focal solid portion within the tumor mass. The case reported here is one of a completely cystic mass. To our knowledge, only 3 such cases have been previously reported: one involving the cervical region and the other two involving the lumbar region (4, 6, 8).
The diagnosis of purely cystic spinal schwannoma is difficult because of its rarity. Therefore, this tumor type needs to be considered with differential diagnosis of cystic spinal lesions, including dermoid cysts, epidermoid cysts, arachnoid cysts, neurenteric cysts, cystic teratomas, meningoceles, primary bone cysts or cystic tumors, and perineural cysts. MRI can be useful in the differentiation of cystic schwannomas from other spinal cystic masses (3, 6, 8).
The treatment strategies for cystic giant spinal schwannomas are not different from those for typical schwannomas. Furthermore, the prognosis is good for the cystic giant spinal schwannomas and it is comparable to that of the solid spinal schwannomas (3, 7, 10).
The complete resection is the treatment of choice, as residual tumor is likely to regrow, increasing the risk of surgical complications due to the repeat operations. However, in cases of the giant invasive spinal schwannomas, a complete tumor resection is difficult because of the invasive tumor growth in all directions. The risk of neurological deficit and surgery-related complications is relatively high on this account. Therefore, the best option is to attempt to achieve a complete resection, but if this is too difficult or risky, removal should be performed to the maximum extent as possible. The measurement of the Ki-67 index and MRI should be performed as follow-up evaluations for the sequential assessment of tumor progression. The Ki-67 index is useful for predicting tumor regrowth or recurrence when complete resection is not achieved (10).
In conclusion, the giant spinal schwannomas with complete cystic degeneration are very rare, but this tumor type should be considered in the cases of cystic sacral masses. In these cases, careful evaluation of the anatomic relation of the tumor is important. In our case, the distinction between bone cyst with hemorrhage and cystic schwannoma was difficult, but the relation to the nerve root provided a decisive clue. The role of a radiologist is crucial in making the surgeons aware of different pathologies in the cases of sacral tumors, thereby helping them to decide on the extent of surgical removal, based on MRI findings in conjunction with intraoperative findings.


 XML Download
XML Download