

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A plexiform angiomyxoid myofibroblastic tumor (PAMT) is a recently described and extremely rare mesenchymal tumor of the stomach. Only 24 cases have been reported in the English literature (1-10) since it was first described by Takahashi et al. (1) in 2007. This tumor is characterized by a plexiform nodular growth of bland spindle cells in the myxoid or fibromyxoid stroma.
PAMT is a benign gastric neoplasm with clinicopathological characteristics that are distinct from gastrointestinal stromal tumors and other mesenchymal tumors of the stomach.
Here, we describe a case of PAMT presenting with a subepithelial gastric tumor detected on preoperative endoscopy, and we also present data from multi-detector computed tomography (MDCT) and a review of the literature.
CASE REPORT
A 38-year-old woman with the clinical impression of a subepithelial tumor of the stomach, which was detected during a health screening examination, visited the Inje University Haeundae Paik Hospital for further evaluation of the lesion. A MDCT scan was performed to characterize the focal gastric lesion. MDCT included an arterial phase scan and a portal phase scan with a 30° left posterior oblique position for appropriate distension and preparation of the lower two-thirds of the stomach, as well as a delayed scan in the right decubitus position for better visualization of the gastric fundus.
Arterial, portal phase, and delayed phase scans were followed with a 15-s delay after attenuation of the aorta at the thoracolumbar junction had reached 100 Hounsfield unit and a fixed 70-s delay, 120-s delay, respectively, after the intravenous injection of 150 mL of iopromide (Ultravist 370; Bayer Schering Pharma, Berlin, Germany) administered at a rate of 3 mL/s with an autonomic injector.
The MDCT scan demonstrated a 3.5 × 2.3 cm-sized polypoid mass with prominent contrast enhancement in the high body along the greater curvature (Fig. 1A-C). The enhancement pattern was heterogeneous. Some portions demonstrated highly vascular prominent enhancement, while other portions showed lesser degrees of enhancement. No enlargement of any lymph node was observed in the regional or distant area. Upon endoscopy, a 3.5 × 2.3 cm sized luminal protruding polypoid subepithelial tumor lesion with central mucosal ulceration was found at the upper body, posterior wall and greater curvature side of the stomach (Fig. 1D).
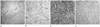
A wedge resection was performed given the sufficient margin. The tumor was an unencapsulated soft tissue mass located at the submucosal layer of the stomach. The resected specimen contained mucinous material within the mass. The tumor was microscopically characterized on low power by a multinodular plexiform growth pattern (Fig. 2A). The tumor cells were bland spindle cells in the myxoid stroma with abundant small blood vessels (Fig. 2B). The tumor cells were positive for smooth muscle actin (SMA) (Fig. 2C), and a special stain for Alcian blue (Fig. 2D) showed a positive reaction in the myxoid stroma. Additional immunohistochemistry for CD117 (c-KIT), CD34, and S-100 proteins were negative in the tumor cells, excluding the possibility of a gastrointestinal stromal tumor (GIST) or neurogenic tumor. Based on the characteristic multinodular plexiform growth pattern, bland spindle cells, positive-form SMA and Alcian blue-positive myxoid stroma rich in small vessels, the gastric tumor was diagnosed as PAMT of the stomach. The postoperative course was uneventful, and the patient is alive without any recurrence or metastasis of the tumor after a 6-month follow-up.
DISCUSSION
PAMT of the stomach is a recently described unique gastric mesenchymal tumor that is myofibroblastic in origin and has the potential to differentiate into smooth muscle cells. The tumor cells are bland and plexiform-arranged in a myxoid stroma. The diagnosis of PAMT is based on the histological feature of plexiform architecture, an abundant myxoid stroma rich in small blood vessels, and immunohistochemical findings. Reported cases fall under the various diagnostic names of "PAMT" (1, 2), "plexiform fibromyxoma" (3), and "plexiform angiomyxoid tumor"(4), and almost all cases have focused on a pathological review. This case is the first report to focus on radiologic findings.
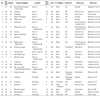
Table 1 summarizes the clinicoradiological features of the previously reported cases, including our unpublished case. To date, there is no sex predilection, and the tumors have occurred over a wide range of ages (7-75 years, mean; 44 years). PAMTs range in size from 1.5 to 15 cm with a mean of 5.5 cm. A very characteristic feature is its common location in the gastric antrum (1-5, 8-10). The tumor can extend to the pylorus and may also involve the duodenal bulb. However, PAMTs can occur anywhere in the stomach, including the fundus (6) or body (7), similar to our case. Ulceration or gastrointestinal bleeding is a common clinical presentation, and two cases of gastric perforation have been reported (1, 5). The surface of the tumor is eroded or ulcerated in approximately two-thirds of cases. The gross appearance resembles a lobulated, sometimes multinodular, white, red, or brown submucosal or transmural mass. Rather than projecting intraluminally, the mass often protrudes toward the serosal surface. CT findings have been described in only three cases, including the present case; one other case demonstrated prominent enhancement, but the other showed poor enhancement, conflicting with the first. We expect that a PAMT would be relatively well enhanced on a CT scan, as the stroma is rich in small vessels; however, the reported data are insufficient to reach this conclusion.
Distal or partial gastrectomy, wedge resection, and even endoscopic resection (6, 7) are performed for treatment. If preoperative endoscopic tissue sampling is accurately performed, the tumor can be treated by endoscopic resection. In all 24 reported cases to date, no recurrence or metastasis of the disease has occurred, although tumors have reached a size of up to 15 cm at its greatest dimension (3).
Nevertheless, the follow-up duration was too short in some cases to precisely predict the prognosis. Although the number of reported PAMT cases is small, malignant changes, metastasis to adjacent organs, and recurrence or death from disease have not yet been reported; therefore, it has been regarded as a benign tumor.
Radiological differential diagnosis of this disease entity includes GIST, leiomyoma, schwannoma, well-differentiated gastric endocrine tumor, ectopic pancreas, and inflammatory fibroid polyp. Because all of these neoplasms arise in the gastric wall, their radiological features may be similar. Because a GIST is the most common subepithelial tumor of the stomach, other subepithelial tumors can be mistaken for a GIST. Many studies have reported imaging findings of benign subepithelial tumors distinguished from GISTs by their potential malignancy (11-17).
GIST is the most common subepithelial tumor of the stomach, and the incidence of PAMT is estimated by Miettinen et al. (3) at less than 1 in 150 compared with that of gastric GIST. In our case, as the tumor was located in the submucosa and proper muscle layer, the most important differential diagnosis was GIST. Most cases of GIST occur in patients > 50 years of age at the time of presentation, and GISTs are rarely observed in patients < 40 years of age (11). The tumors have a smooth mucosal surface and are generally intact in the overlying mucosal surface, with exception of the focal areas of ulceration. GISTs mainly present as an extragastric extension of the tumor, approximately 86% into the gastrohepatic ligament, gastrosplenic ligament or lesser sac. A focal intraluminal polypoid mass resembling a mucosal polyp is the least common appearance of GISTs, representing approximately 14% of the GISTs (12). GISTs consist of spindle cells that are arranged in short fascicles and/or epithelioid cells that are arranged in organoid clusters or sheets (1). GIST does not show a distinctive plexiform intramural growth pattern, and PAMTs have less eosinophilic cytoplasm than GISTs. Moreover, compared to the tumor cell populations found in GIST, the stromal component is prominent; the immunohistochemistry of PAMT is clearly distinguished from GIST, being negative for CD117 (c-KIT) and CD34. Approximately 90% of GISTs are positive for CD117 (c-KIT) immunohistochemically.
Gastric leiomyoma is the second most common subepithelial gastric tumor and particularly frequently develops in the gastric cardia and high body. Thus, another important differential diagnosis in this case is gastric leiomyoma. Mainly, gastric leiomyomas shows a lobulated, contoured, protruding luminal mass mimicking the present case, but the mass manifests as poorly enhanced and homogeneously correlated with the liver, unlike our case, and is rarely in combination with surface ulcerations (13). Gastric leiomyoma is characterized by the fascicular arrangement of tumor cells that possess spindle-shaped nuclei and markedly eosinophilic cytoplasm (1). Leiomyomas are positive for SMA, desmin, and focally for CD34.
Gastric schwannoma is histologically characterized by long fascicular arrangements of bundled spindle cells that often have a distinctive lymphoid cuff, which may contain germinal centers and stain positive for S-100. Although small gastric schwannomas and GISTs show similar imaging findings.
Well-differentiated gastric neuroendocrine tumors (carcinoids) are most commonly observed in the gastric antrum and manifest as one or more small intraluminal subepithelial masses with a characteristic central ulceration, which was consistent with the present case (15). They are manifested as avid enhancement in the early phase of dynamic contrast-enhanced CT, and consequently, they are less prominent in the portal venous and equilibrium phases. They have a small-sized monotonous neuroendocrine cell nest that histologically suggests a population of neuroendocrine tumors, with abundant cytoplasm and round, smooth-contoured nuclei. Immunohistological staining for chromogranin and synaptophysin also suggest a neuroendocrine tumor.
Gastric glomus tumors are exclusively manifested at the gastric antrum and show peripheral nodular or strong homogeneous enhancing vascular tumors in the arterial phase and prolonged enhancement in the delayed phase (16). Characteristically, these tumors have thicker normal overlying mucosa than other subepithelial gastric tumors and are immunohistochemically positive for CD34 and SMA. PAMT may be a well enhanced tumor due to the numerous small blood vessels observed in the myxoid stroma; hence, it is able to mimic vascular tumors.
An ectopic pancreas is another example of an intraluminal protruding tumor that is manifested with good enhancement; these appear as pancreatic tissue that contains the central umbilicus. However, most ectopic pancreases develop at the gastric antrum within 3 cm from the pylorus and demonstrate oval or flat tumors (17).
Inflammatory fibroid polyps are rare, benign, tumor-like lesions of the gastrointestinal tract. They are most commonly localized to the gastric antrum, usually present in the sixth or seventh decade, but arise from the submucosa and project into the bowel lumen. As in the present case, the mucosal surface is usually ulcerated. These polyps are composed of epithelioid- to spindle-shaped fibroblast proliferations in an onion-skin like pattern around the vessels and are infiltrated with inflammatory cells such as eosinophils, lymphocytes, macrophages, and mastocytes. The present case showed a lack of this infiltration by inflammatory cells, distinguishing it from a case of inflammatory fibroid polyps. All types of gastric subepithelial tumors except for GISTs are negative for CD117 (c-KIT). Inflammatory fibroid polyps are usually positive for CD34, and GIST, leiomyoma, glomus tumor, and schwannoma show focally positivity for CD34, but this PAMT case was negative for CD34; therefore, this present case could be distinguished from an inflammatory fibroid polyp immunohistologically.
In conclusion, we described a case of PAMT, a rarely reported distinctive benign subepithelial tumor of the stomach. This tumor is characterized by its common combination with mucosal surface ulceration, heterogeneously prominent enhancement, and antral involvement (although not observed in the present case). Signs of this tumor indicate the histological characterization of a multinodular plexiform growth pattern, proliferation of bland spindle cells, and the numerous small blood vessels observed in the myxoid stroma. The myofibroblastic nature of the tumor cells was confirmed by immunohistochemistry. In general, PAMT tumor cells are positive for SMA, and the myxoid stromal matrix is positive for Alcian blue. These histological and immunohistochemical features are helpful when diagnosing this rare disease. Our report may help to increase the awareness of this rare but important new disease entity.

 XML Download
XML Download