

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The incidence of bilateral breast cancer has been reported to range from 0.4% to 14% (1, 2). Several studies have reported that contralateral cancer was small and could frequently be detected on mammography (3).
Here, we report a case of metachronous bilateral breast cancer that developed 5 years after the occurrence of ipsilateral breast cancer. To the best of our knowledge, no cases of metachronous bilateral breast cancer with bilateral recurrence have been previously reported in the literature.
CASE REPORT
In October 2009, a 51-year-old female complained of swelling in her right breast. She had a history of a bilateral partial mastectomy (PM) due to a previous occurrence of the bilateral breast cancer. The patient's past medical history was as follows. In August 1999, she underwent a right upper medial PM for an invasive ductal carcinoma (IDC). Following the surgical procedure, she received radiotherapy. Annual follow-up mammograms and ultrasound revealed no suspicious lesions until 2003. In October 2004, she underwent a left upper outer PM, after a mixed tubular carcinoma was discovered during the surveillance. For five years after the surgery, no evidence of recurrence or metastatic lesions was observed during the follow-up examinations, until newly developed microcalcifications were found in the right breast in 2009.
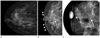
Compared to the mammographic findings from July 2009, which was only 3 months prior, this mammography showed increased pleomorphic microcalcification with segmental distribution in the right upper medial breast, which extended to the right subareolar area, and the skin thickening or trabecular thickening, in the right medial breast (Fig. 1). These microcalcifications were categorized as Breast Imaging-Reporting and Data System (BI-RADS) category 4b (4). Stereotactic vacuum-assisted biopsy was recommended. However a punch biopsy of the skin in the periareolar area was performed based on the physician's discretion. The pathology results revealed adenocarcinoma with lymphatic emboli, which means invasion of the skin dermal lymphatics by breast cancer cells consistent with inflammatory breast cancer. The patient didn't receive left mammogram at that time. She underwent fluorine-18 fluorodeoxyglucose for detecting distant metastases and negative results. The patient underwent a right modified radical mastectomy (MRM) and the pathologic review revealed the multifocal IDC.
During surveillance after the right MRM in April 2011, the left mammogram was compared to mammography performed only 6 month prior, which was October 2010. The left mammogram showed an increased pleomorphic microcalcification with segmental distribution in the left upper central quadrant, assessed as BI-RADS category 4c (Fig. 2) (4). Based on the patient's preference, she underwent a left MRM without biopsy. The final pathologic review revealed multifocal IDC.
DISCUSSION
The incidence of bilateral primary breast carcinoma has been gradually increasing as a result of improved early detection capabilities and longer survival times (5). The incidence of bilateral breast cancer has been reported to range from 0.4% to 14% (1, 2). The prevalence of synchronous bilateral cancer is approximately 1-3%, and the prevalence of metachronous breast cancer is 5-7% (6). The risk factors for bilateral breast cancer are variable. The heredity in breast cancers is the most significant factor for an increased risk of developing bilateral breast cancer. Other factors associated with an increased risk of bilateral breast cancer include familial breast cancer, radiation exposure at young age, lobular carcinoma in situ, lobular invasive carcinoma, and multicentric cancer (7). Among women of age less than 45 years at the time of irradiation, the overall relative risk of contralateral breast cancer was increased by 1.6 (95% confidence interval, 1.1-2.4) times after the radiation therapy (8). A diagnosis of the primary breast cancer at a young age is also associated with an increased susceptibility for bilateral breast cancer. This is mainly due to the increased likelihood of living long enough to develop a metachronous breast cancer, with twenty-five year cumulative risk of 6.9% (8). Our patient had the above-mentioned risk factors-primary breast cancer and radiation exposure at a young age-for bilateral breast cancer.
Takahashi et al. (1) reported that the median period, between the development of the first and second primary carcinomas in metachronous cases, was 113.0 months with both 5 and 10 years of disease-free survival rates as 65.0%. Our case of metachronous bilateral breast cancer had a disease-free survival time of 62 months. This patient had undergone a bilateral partial mastectomy, and her personal history of breast cancer placed her at high risk for recurrence. The bilateral recurrences after bilateral partial mastectomy, manifested as microcalcifications, developed in 3 months in the right breast and 6 months in the left breast. She has received continuous surveillance after the surgery. Cowan et al. (9) suggested that the rapid tumor growth is associated with the failure to detect breast cancer by mammography. However, in the present case, we immediately detected suspicious microcalcifications on mammography. The short-interval mammography, of less than 6 months after breast-conserving treatment, has not previously been reported. In our case, as the patient complained of discomfort and swelling in her breast, probably due to the very rapid growth of tumor, a mammogram was performed only 3 months after the previous mammogram.
The effective trials to detect contralateral metachronous breast cancer, using various modalities besides mammography, have been done (10). Robertson et al. (10) reported that MRI has a higher diagnostic value than the surveillance mammography, in the women previously treated for primary breast cancer.
Herein, we report a case of bilateral metachronous breast cancer with ultimate bilateral recurrences. Our case suggested that the primary breast cancer and radiation exposure at a young age might be associated with an increased risk of the bilateral breast cancer.

 XML Download
XML Download