

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A tuberculous aortic aneurysm is a rare condition. Multiple tuberculous aneurysms of the aorta are extremely rare and fewer than five cases have been reported (1, 2, 3, 4). If patients with a tuberculous aortic aneurysm are not treated properly, they may die due to aneurysm rupture. In the past, surgery was the standard treatment option for tuberculous aortic aneurysm, but it carries a high risk of mortality and morbidity. Endovascular stent graft is an emerging treatment option for tuberculous aortic aneurysm and can replace surgery in some cases (5, 6, 7). However, no reports of endovascular stent graft repair for multiple tuberculous aneurysms of the aorta are available. Herein, we report a case of successful treatment of multiple tuberculous aneurysms of both the thoracic and abdominal aortas using an endovascular stent graft, combined with antimycobacterial treatment.
CASE REPORT
A 47-year-old man was admitted to our hospital for further evaluation of persistent fever. He had left buttock abscess, left inguinal lymphadenitis and fever for the past 5 months despite conservative management at another hospital. An ultrasonography-guided gun biopsy from the inguinal lymph node showed a positive result on the Mycobacterium tuberculosis-polymerase chain reaction assay.
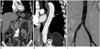
Contrast-enhanced pelvic computed tomography (CT) was performed to evaluate the left buttock abscess. The CT showed that the left buttock abscess had almost resolved, but it revealed 22-mm and 7-mm saccular pseudoaneurysms of the infrarenal abdominal aorta and a 27-mm saccular pseudoaneurysm of the right common iliac artery. Despite one month of antimycobacterial treatment, a follow-up CT scan showed that one of the pseudoaneurysms of the infrarenal abdominal aorta had increased in diameter from 22-mm to 34-mm. The CT also revealed a newly developed 7 mm saccular pseudoaneurysm of the descending thoracic aorta (Fig. 1A, B). Because CT scans of the patient had little evidence of active infection such as adjacent soft-tissue mass, fat stranding or fluid in a unusual location, the patient was considered for the endovascular treatment (8).
The patient underwent endovascular repair of the pseudoaneurysms at the aortoiliac bifurcation. A bifurcated stent graft (Medtronic, Minneapolis, MN, USA) was placed without any immediate complication. Completion angiography showed a type II endoleak at the right side of the lower abdominal aorta, although the two pseudoaneurysms of the aortoiliac bifurcation were completely excluded (Fig. 1C). A 1 month follow-up, CT scan demonstrated that the type II endoleak was persistent. Moreover, the pseudoaneurysm of the descending thoracic aorta had increased in diameter from 7-mm to 15-mm.
Transcatheter embolization was performed via the transabdominal approach to repair the endoleak in the lower abdominal aorta (Fig. 2A). The endoleak cavity was directly punctured percutaneously using a 22-gauge needle under fluoroscopic and ultrasound guidance. Then, contrast agent was injected through the puncture needle to evaluate the endoleak cavity and demonstrated that the cavity was supplied from the left fourth lumbar artery. Embolization of the feeding artery was successfully accomplished using a 1:1 mixture of glue and Lipiodol. An endovascular stent graft (Medtronic, Minneapolis, MN, USA) was placed correctly to treat the pseudoaneurysm of the descending thoracic aorta. No immediate complications occurred after the procedure (Fig. 2B).
CT scans at 3 and 8 weeks after the procedure demonstrated that the two stent grafts were placed properly with complete exclusion of the pseudoaneurysms and the endoleak had completely resolved. The patient continued antimycobacterial treatment for 1 year and no longer had a fever 2 months after the procedure. Fourteen months after the procedure, the patient was stable and there was no recurrence on imaging follow-up (Fig. 3).
DISCUSSION
The incidence of a tuberculous aneurysm of the aorta is very low. About 100 case reports have been published and multiple tuberculous aneurysms of both the thoracic and abdominal aorta are exceptional (1). The natural course of an untreated tuberculous aortic aneurysm is very unfavorable due to aneurysmal rupture and it is not dependent on lesion size. Most tuberculous aneurysms are false, saccular aneurysms and are most common in the thoracic aorta.
Successful treatment of a tuberculous pseudoaneurysm always includes both medical and surgical treatment (9, 10). In one review article, patient mortality increased when treated only by medical or surgical therapy (9). Surgery is part of a standard treatment plan, but it has been associated with a high risk of mortality and morbidity. Therefore, endovascular treatment is considered a current trend and has replaced surgical therapy (5, 6, 7).
Endovascular repair can be the first-line treatment option in selected patients with a tuberculous aortic aneurysm. First, this type of repair should be considered in debilitated patients because of high risk for major complications after surgery. Second, patients with minimally infected tissue would be indicated (8). Third, patients who have limited life expectancy should be considered for palliative treatment (11). Finally, it could also be considered in a patient with a ruptured aneurysm (7).
If active infection or aortoenteric fistula of the patient are evident, there is a high risk for recurrence of infection after the procedure. Therefore, patients who have extensive infection are preferably excluded from endovascular repair. In our case, the endovascular option was considered because the infection was minimal and localized on the CT scan, and the general condition of our patient was relatively stable.
Continued antimycobacterial therapy is required with endovascular treatment. Antituberculous drugs after surgery should be continued from 9 to 12 months, furthermore some advocates indefinite use of antituberculous drugs (1). Therefore, antimycobacterial therapy after endovascular treatment should be continued at least 9 months.
Less than five cases of multiple tuberculous aortic aneurysms have been reported (1, 2, 3, 4). Surgical treatment was performed in three reports and a 16-year-old girl was treated with a multi-layered stent. However, no reports are available on multiple tuberculous aneurysms of both thoracic and abdominal aorta treated with an endovascular stent graft.
In summary, endovascular stent graft repair was successful in a patient with multiple aneurysms of the descending thoracic and abdominal aorta as well as the right common iliac artery. No recurrence was evident 14 months after the procedure.


 XML Download
XML Download