

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The liver has a unique anatomy and physiology which allows for liver procurement from a living donor. Because of recent advances in surgical techniques, living-donor liver transplantation (LDLT) in adults is being performed with increasing frequency and is considered as the treatment of choice for end-stage liver disease (1, 2). Living donor hepatectomy offers an exclusive insight into liver regeneration in normal livers (3-6). In healthy donors, up to 75% of the whole liver volume can be donated (1, 2). However, donation of the partial liver is not without risk for donors. The risk for donors increases with increase of the graft volume. Because donor safety is paramount in LDLT, knowledge about the postoperative changes in the donor's remnant liver and spleen is important. Because of the ability of the liver to regenerate, both the transplanted graft and the remaining liver are expected to regenerate and compensate for the loss of hepatic volume in the recipient and donor, respectively. It has been well documented that remnant liver enlargement occurs in the postoperative period following partial liver donation (7). The spleen also enlarges following major hepatic resection and after liver donation (7-9). To explain this phenomenon, relative portal hypertension (increase of the portal pressure after donor hepatectomy as compared with the preoperative state) and elevation in the levels of growth factors have been postulated as causes (10). However, the exact mechanism of the increase in the liver and spleen volume has not been completely elucidated. A direct correlation between the portal pressure and volume changes in the liver and spleen has not been reported. Therefore, we attempted to delineate liver and spleen volume changes during the early postoperative period 2 weeks after surgery and tried to identify possible influencing factors, including portal venous pressure changes, of the liver and spleen volume changes.
MATERIALS AND METHODS
Patients and Surgical Record Review
Institutional review board approval was obtained and the requirement for informed patient consent was waived for this retrospective study. Review of the electronic medical record database and surgical record database of our institution revealed 27 LDLT between September 2001 and November 2005. During this period, intraoperative measurement of the portal venous pressure before and after donor hepatectomy was routinely performed. A total of 27 donor hepatectomies were performed in 27 patients during this period. There were 23 men and 4 women. The mean age of the patients was 32.7 years old (age range, 17-54 years old). Right hemihepatectomy was performed in 24 patients. In 7 patients with right hemihepatectomy, the middle hepatic vein was included in the transplant. Extended right hemihepatectomy was performed in 3 patients.
The patients' electronic medical records and surgical records were reviewed to find relevant data including the plasma indocyanine green (ICG) retention rate at 15 minutes after ICG administration (ICG R15), preoperative platelet count, resected liver volume, and the portal venous pressure measured before (PV0) and after (PV1) hepatectomy. The percent change in the portal venous pressure was defined as (PV1 - PV0) × 100 / PV0. The resected liver volume was calculated based on the assumption that the mean density of healthy liver tissue was 1.00 g/mL (11).
CT Scans and CT Volumetry
At our institution, multi-detector row helical computed tomography (MDCT) is routinely used for preoperative imaging evaluation of LDLT donors. After donor hepatectomy, donors are regularly followed-up at 2 weeks after hepatectomy with an MDCT. All CT scans were performed with a 16-channel MDCT scanner (Lightspeed 16; GE Healthcare, Milwaukee, WI, USA). Non-enhanced CT scans were performed first. For dynamic contrast-enhanced CT, 2 mg/kg of a non-ionic contrast agent (Omnipaque 300; GE Healthcare, Milwaukee, WI, USA) was administrated intravenously at a flow rate of 3 mL/sec using a power injector. Imaging was conducted at three different phases (hepatic arterial dominant, portal venous dominant, and late equilibrium phases) determined by bolus tracking and automated triggering technology. Non-enhanced scans and portal venous dominant phase imaging were obtained from the dome of the diaphragm to the pubic symphysis. The hepatic arterial dominant phase was obtained from the dome of the diaphragm to the iliac crest, to cover the entire liver. The protocol was as follows: 140 kVp; 350 mA; section thickness, 0.625 mm; pitch, 1.75; table speed, 35 mm/sec (17.5 mm per rotation with two rotations); and gantry speed, 0.5 second per rotation. The transverse section data were reconstructed with 5-mm-thick sections at 5-mm intervals in the transverse plane. Coronal reformatted images were reconstructed with 3-mm sections at 3-mm intervals. The 5-mm transverse and 3-mm coronal images were reconstructed at the operator's console and transferred to a picture archiving and communication system (PACS) workstation (INFINITT PACS, Infinitt Co., Ltd, Seoul, Korea) as a separate series of scans for interpretation.
CT volumetry for the whole liver and spleen was performed at PACS workstations by one radiologist with six years of abdominal CT imaging experience (J. B.). Transverse plane images of the portal venous dominant phase were used for the CT volumetry. A manual trace of the contours of all liver and all spleen sections was performed on a PACS viewer with an electronic cursor. The manufacturer's software automatically calculated the number of pixels included within the traced contours for each section and provided the cross-sectional area of each organ on a section-by-section basis. The circumscribed areas were then multiplied by the CT section thickness, yielding an approximate volume for the liver or spleen section, and the volumes of all sections were summed to give the total volume of the liver or spleen.
Statistical Analysis
The remnant liver volume in the immediate postoperative period (LV0) was calculated by subtracting the resected liver volume (LVR) from the preoperative whole liver volume (LVW). The rates of liver volume change and the rate of spleen volume change were defined as [(LV2wks - LV0) / LV0] and [(SV2wks - SV0) / SV0], respectively, where LV2wks is the liver volume at 2 weeks after hepatectomy, LV0 is the remnant liver volume after hepatectomy, SV2wks is the spleen volume at 2 weeks after hepatectomy, and SV0 is the preoperative spleen volume. Volume changes were correlated with several relevant and measurable factors that could influence volume changes. The resected-to-whole liver volume ratio was defined as LVR/LVW, and the resected liver to the sum of the liver and spleen volume ratio was defined as LVR/(LVW + SV0), where LVR is the resected liver volume, LVW is the preoperative whole liver volume, and SV0 is the preoperative spleen volume.
Measured volumetric data and relevant clinical parameters, including ICG R15, preoperative platelet count, measured portal venous pressures and changes in the portal venous pressure, were statistically analyzed to look for correlations. The paired t-test was used to compare the liver and spleen volume before and after donation. In all cases, a p value < 0.05 was considered significant. For statistical analysis, Pearson's correlation analysis was performed by using software (SPSS for Window, version 11.0; SPSS Inc., Chicago, IL, USA).
RESULTS
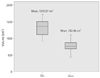
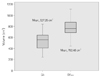
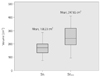
The average whole liver volume (LVW) at donation was 1331.57 ± 225.59 cm3 and the average resected liver volume (LVR) was 801.15 ± 138.29 cm3; the average remnant liver volume immediately after donation (LV0) was 527.25 ± 166.85 cm3, and the liver volume 2 weeks after donation (LV2wks) was 782.48 ± 168.90 cm3 (Fig. 1A, B). The mean liver volume two weeks after hepatectomy in this series was 58.99 ± 9.51% of the original liver volume. The mean liver volume at two weeks after hepatectomy was significantly lower than that of the original liver volume (p < 0.01) (Fig. 2). In all hepatectomy donors, the remnant liver showed an increment of the volume two weeks after hepatectomy (p < 0.01) (Fig. 3). The increment rate of the remnant liver volume was 59.45 ± 50.52% (Table 1). The average spleen volume at donation (SV0) was 168.23 ± 54.31 cm3 and the average spleen volume two weeks after donation (SV2wks) was 247.65 ± 86.33 cm3 (Fig. 1C, D). There was a statistically significant increment in the splenic volume in donors two weeks post-donation (p < 0.01), with a mean increment of splenic size of 47.94 ± 22.61% (Table 1) (Fig. 4). The mean platelet count of donors at donation (PLT0) was 255.54 × 103/mm3 (normal range 150-400 × 103/mm3), and the mean platelet count at 2 weeks (PLT2wks) was 268.12 × 103/mm3. There was no statistical significance difference in platelet levels pre-donation and at 2 weeks post-donation (Table 1).
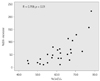
The remnant liver volume increment rate revealed a positive correlation with the resected-to-whole liver volume ratio (LVR/LVW) (r = 0.759, p < 0.01) (Fig. 5). The other analyzed factors, including portal venous pressure, showed no correlation with the changes of the liver and spleen volumes (Table 2).
DISCUSSION
The liver has the ability to self-regenerate when there is loss of functional liver tissue. This property of the liver and recent advances in surgical techniques have made LDLT feasible (1, 2). LDLT can alleviate the problem of organ shortage that is due to a markedly limited cadaveric donor supply, and it can reduce mortality while patients are on the waiting list. In adult patients, a right lobe graft is mainly used to cope with the volume requirement for the recipient. The capability of the liver to regenerate provides great advantages for living donor liver transplantation compared with living related kidney transplantation (12). However, the process of regeneration is a complex one and it is still not completely understood (7). There have been many studies on the regeneration of the liver after hepatectomy, but these have been done in diseased livers, and their results cannot be applied directly to living donor hepatectomy (13). The liver after liver resection for benign diseases of the liver can be a model for liver regeneration in normal human livers (14). Greene et al. (15) demonstrated with an animal model experiment that endothelial cells are involved in the regulation of the regenerating adult liver, and they suggested that angiogenesis controls the regenerative process. After a partial hepactectomy, massive hepatocyte proliferation is observed to begin immediately, peaking at 48 hours postoperatively. Endothelial cells, on the other hand, lag behind and peak only 4 days after the operation proper (15). In our series, the mean liver volume as measured 2 weeks after hepatectomy was 58.99 ± 9.41% of the original liver volume. This percentage was significantly lower when compared to the pre-donation volumes overall in all donors. Ibrahim et al. (7) reported that full liver regeneration was not attained at 6 months after donation in most donors. Some authors believe that the liver will enter into a slower pace of regeneration once it reaches an adequate hepatocyte mass to support normal metabolism (4-6, 16). In this study, the increment rate of the remnant liver volume showed a wide range (59.45 ± 50.52%). One of the patients in this study more than doubled their liver volume (222%) by 2 weeks after donor hepatectomy. In this patient, the resected-to-whole liver volume ratio (LVR/LVW) was the highest among the included patients (78.2%). Therefore, we presume this exceptionally high resected-to-whole liver volume is the cause of the extremely high rate of volume increase.
Our study showed that the volume increment rate of the remnant liver 2 weeks after partial liver donation correlated not with the absolute resected liver volume (LVR) but with the relative resected liver volume compared to the whole liver (LVR/LVW). These results suggest that the trigger for liver regeneration may be the relative shortage of liver tissue for supporting normal metabolism. However, our study showed that there was no correlation between portal venous pressure and the volume increment of the remnant liver. This result suggests that relative portal hypertension is not a major factor in triggering liver regeneration. According to recent other studies, we presume that some other complex mechanism including humoral factors such as growth factors, including epidermal growth factor, and transforming growth factor-a, are involved in the process.
It has been known that there is splenic enlargement in patients who undergo liver resection (7-9). This enlargement was most marked in patients with liver cirrhosis in whom hypersplenism can be detrimental (9). Ando et al. (10) showed that the spleen enlarges as much as 155 ± 40% within 14 days after hepatectomy for biliary cancer. It has been conventionally conjectured that the spleen enlarges as a consequence of relative portal hypertension, and that the enlargement is simply a reflection of splenic engorgement (17). The results of several recent animal studies indicate that both the liver and spleen respond to the same growth factors, epidermal growth factor, transforming growth factor-a, or perhaps a combination of these factors (18-21). In humans, the relationship between splenic enlargement and post-hepatectomy is rather complex and controversial. Ando et al. (10) recently found that the increment in the splenic volume correlated well with the increment in the remnant liver volume and suggested the presence of a common growth factor. Sato et al. (22), on the other hand, suggested that the percent increase in liver volume was inversely related to the spleen volume. Both of the above studies were done in diseased livers with underlying parenchymal disease. Ibrahim et al. (7) reported that the spleen enlarges as the liver regenerates after donor hepatectomy. Ibrahim et al. (7) also reported that there was a strong correlation between the amount of the resected liver tissue and the size of the splenic enlargement. This favors the hypothesis that both organs are stimulated by the same growth factor, and in some donors, this process seems to be more active leading to greater enlargement of both the spleen and liver. However, our study results showed no correlation between the volume increment rate of the remnant liver and that of the spleen. Furthermore, the volume increment ratio of the spleen did not show any correlation with the portal venous pressures measured during the surgery, before clamping and after declamping of the main portal vein. We believe that these discrepancies could be explained by the multifactorial nature of liver and spleen regeneration. Liver and spleen regeneration is not affected by a single factor but by many different physiological and anatomical ones that together form a web of complex relationships (7).
Our study has some limitations. Our study data was small, and only 27 cases were reviewed. Because this was a retrospective analysis, there could be other factors such as growth factors acting on the liver and spleen causing volume enlargement or humoral factors that were not assessed in this series. One possible relevant factor is the change in the donors' body weight before donation and 2 weeks after. This factor cannot be analyzed because there was no data on the donors' body weight at 2 weeks post-donation in the electronic medical record database.
In conclusion, the spleen and remnant liver volumes were increased at CT volumetry performed 2 weeks after partial liver donation. Remnant liver regeneration after liver donation is correlated with the relative resected liver volume as compared to the whole liver volume. The other analyzed factors, including the portal venous pressure, were not correlated with the liver or spleen volume changes. Liver and spleen regeneration is a highly complex process in humans. Many factors play a part in the physiological regeneration of the liver and spleen. More studies are warranted to define the possible presence of any other factors that affect the rate of splenic regeneration. This would be useful both for candidates involved in liver donation as well as for patients undergoing other forms of hepatic surgery.



 XML Download
XML Download