

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The distal tibia is the second most common site of physeal fracture, followed by the distal radius (1). Salter-Harris (S-H) type I fracture has been considered as a low-grade physeal injury and usually needs conservative management with closed reduction and immobilization (2). However, although not commonly seen, soft tissue structures, including periosteum, tendons and ligaments, can be interposed in the physis, and it has been associated with subsequent growth disturbances and requires open surgical reductions to remove the entrapped structures (3-5). Particularly, interposed periosteum in the physis has been reported as the most common cause of failed closed reductions (3-5). Although irreducible fractures of the physis due to interposed soft tissues have been reported in the orthopedic literature, there are only a few reports concerning the preoperative magnetic resonance (MR) imaging diagnosis. We report MR imaging findings of distal tibial S-H type I fracture with periosteal interposition, which underwent open surgical reduction.
CASE REPORT
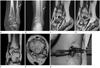
A 10-year-old girl was being presented with a distal lower left extremity injury by a traffic accident. Initial CT scans of the left ankle demonstrated a widening of the medial aspect of the distal tibial physis, which was consistent with Salter-Harris type I fracture and fracture of distal shaft of the fibula (Fig. 1A). Closed reduction with immobilization was performed. Subsequent plain radiographs showed physeal widening (4 mm width) of medial portion of the distal tibia one month later (Fig. 1B). The possibility of soft tissue entrapment within the fractured physis of the distal tibia was considered, and MR imaging was performed. MR imaging of the left ankle demonstrated a linear low signal structure on T2-weighted images extended into the widened physis of anteromedial portion of the distal tibia and surrounding intermediate to low signal lesion (Fig. 1C-F). These lesions were interpreted as an entrapment of torn displaced periosteum within the fractured physis and the surrounding granulation tissues.
Subsequently, she underwent open surgical reduction. At surgery, trapped periosteum within the widened physis was identified in an anteromedial aspect of the distal tibial physis, and fibrous or granulation tissues were filled in the widened physis. These lesions were removed. After the removal of the entrapped periosteum, a widening of the distal tibial physis was noted up to a width of 4 mm (Fig. 1G). A diagnosis of periosteal interposition in distal tibial S-H type I fracture was confirmed.
DISCUSSION
Ankle fractures account for approximately 15% of physeal injuries and the overall incidence of physeal complications after physeal fracture has been reported to be between 2% and 14.1% (2, 6). S-H type I fractures account for approximately 15% of distal tibia physeal fractures (2). While S-H type I fracture has been previously considered as a low-risk injury, a high incidence of premature physeal closure was reported with a rate of 22% to 36% in the few recent studies (4, 6).
Multiple factors proposed as influencing rates of growth disturbances included fracture type and location, displacement, energy of injury, patient's remaining growth potential (age and skeletal maturity) and quality of reduction (4, 6). Also, entrapped periosteum has been described as one of the common causes for irreducible fractures of the distal tibia (5). Other soft tissue structures, such as muscles, tendons and ligaments, also result in irreducibility by trapping in the physeal injury site (5). Studies in animal models have reported that the combination of physeal cartilage injury with periosteal interposition produces poor organizations of the remaining physeal growth plate; thus, producing increased risks of physeal bar formation and also showed significant growth disturbances as compared with fractures of the intact physes (7, 8).
Plain radiography is the initial modality to evaluate physeal injuries and could be sufficient in majority of the cases. In a previous study, it has been reported that the radiographic presence of post-reduction residual physeal gap in S-H type I and II fractures of the distal tibia could suggest interposed periosteum (4). In their study, a gap of more than 3 mm on anteroposterior or lateral radiograph was identified as positive, and their result showed a 3.5-fold increase in the incidence of premature physeal closure, if a gap was presented on the postreduction radiography in S-H type I and II fractures (5). In our case, the residual gap measured as 4 mm on an anteroposterior radiograph, was followed up one month after a closed reduction. The findings in our case suggest the possibility of interposed periosteum within the fractured physis.
MR imaging can clearly demonstrate the morphology, signal intensity of the physis, as well as the relationship between the physis and surrounding structures (9). In a previous study, it has been reported that physeal injury was presented as a low signal intensity, which was similar to the normal physis, on T1-weighted imaging; and as a high signal intensity, which was different from an intermediate signal intensity of the normal physis, on T2-weighted imaging (9). Also, MR imaging has been used for detecting patterns of growth plate injury not depicted on a plain-film, particularly in S-H type I and V fractures (3). Soft tissue entrapments, especially periosteal interposition in physeal fractures, can be demonstrated as linear low signal intensity structures within the widened physis on proton density weighted images with or with156out fat saturation and T2-weighted images (3, 10). MR imaging of ankle in our case also showed entrapped low signal intensity structures within the widened physis on T2-weighted images. However, only a few literatures reported MR imaging findings of trapped periosteum in physeal injury (3, 10).
The usual treatment of S-H type I and II fractures of the distal tibia is closed reduction and immobilization, while S-H type III and IV fractures are treated with open reduction and internal fixation. However, S-H type I and II fractures, which failed with closed reduction, are indications of open surgical reductions. In the orthopedics literature, the most common cause of reduction failure has been recognized as an entrapped periosteum (3). In these cases, open reduction and removal of interposed periosteum in the fractured physis allow for more anatomic reductions and may decrease the incidence of complications, such as non-unions and growth disturbances (4).
The detection of entrapped periosteum with physeal injury on imaging technique is important because perioteal interposition can be the cause of irreducibility and result in complications after physeal fracture. MR imaging can be effective in demonstrating soft tissue entrapments including periosteum or granulation tissue in physeal fractures, as in our case; thereby, allowing a prompt, appropriate operation, which may prevent potential complications.
 XML Download
XML Download