

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The knowledge on the normal anatomy and variation of the internal mammary vessels (IM) is essential to the safety of parasternal percutaneous procedure. A 1995 study by Arnez et al. (1) identified four different patterns of the IMs, with the internal mammary vein (IMV) lying medial to the internal mammary artery (IMA) in 95% of the 34 cadavers (Types 1 and 2) (2). In the 3%, the main trunk of IMV lies lateral to the IMA above the upper border of the second rib, below which it divides into a lateral and medial branch (Type 3); in the remianing 2% (single cadaver), a single-trunk IMV lies lateral to the IMA throughout the parasternal areas (Type 4). To our knowledge, however, the last two patterns have never been demonstrated for cross-sectional imaging to this date. The crossing of the IMA over the IMV has never been reported at the first intercostal space level.
We present two cases of unusual IM course incidentally discovered on the multi-detector CT (MDCT), with the IMV running entirely or laterally to the IMA in the first intercostal space.
CASE REPORT
Case 1
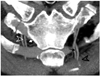
A 25-year-old female is presented with a palpable supraclavicular mass. Neck and chest CT were being obtained for evaluation, which shows a large mass in the anterior mediastinum. The patient is being referred to the radiology department for transthoracic biopsy of the mediastinal mass, when it was noticed that the main trunk of the IMV was running laterally to the IMA on both sides of the mass, at the level of the first intercostal space (Fig. 1A). In the second intercostal space, the left and right IMAs were accompanied by two branches of IMVs lying lateral and medial to each of them. Above the first intercostals space, the IMVs were medial to the IMAs as in most patients, crossing IMAs were near the inferior margin of the first rib.
Although biopsy could be done either medially or laterally to the IMs, the lateral path was chosen to avoid injuries to the IMAs (Fig. 1B). The procedure was uneventful, and the mass was confirmed as a diffused large B cell lymphoma.
Case 2
A 73-year-old male is being presented with cough and sputum that he had suffered for several months. A chest radiograph revealed a cavitary mass in the lower right lobe. The patient is being referred to the radiology department for biopsy of the mass. Diagnostic chest CT was being obtained, which showed an incidental variation of internal mammary vessels: the main 142trunk of the right IMV was running laterally to the IMA in its entire course. The left IMV was running medially to the concomitant IMA in the upper half of the first intercostal space, but was laterally crossed by the IMA in the middle of the intercostal space to the artery at the more caudal levels (Fig. 2). The biopsy was successfully done via a paravertebral approach, yielding the diagnosis of squamous cell carcinoma.
DISCUSSION
Percutaneous transthoracic procedure is actively being performed for evaluation of pulmonary or mediastinal lesions (2). When performing percutaneous procedure via an anterior approach, familiarity to the anatomy of the IMs is essential for the safety of the procedures (3). However, there is a disparity between the results of cadaveric and imaging studies, and whether the IMV runs medially to its concomitant artery in the first or second intercostal space.
In the 1995 cadaveric study, Arnez et al. (1) identified four different types of IM anatomy (Fig. 3): the IMV was found medial to the IMA throughout its course in 95% of cases (Types 1 and 2); In 5% of cases the IMV was lateral to the IMA (Types 3 and 4). According to Arnez et al., the most common arrangement is Type 1: a single IMV lying medial to the IMA divides into two tributaries and is usually at the level of the 3rd or 4th intercostal space. In type 1 (75% of female and 62% of male specimens), the lateral vein crosses anterior to the artery from medial to lateral as it ascends along the sternal margin, and then runs parallel to the artery and the medial vein. In type 2 (22% of female and 31% of male specimens), a single IMV runs medial to the artery throughout its course, with no divisions in the 3rd or 4th intercostal spaces. Types 3 and 4 are rare, with type 4 only found in a single specimen in their study.
On the other hand, no IMVs were found to run laterally to their concomitant IMAs in the 1990 study by Glassberg et al. (3), who reviewed CT of 100 patients. Likewise, a 2003 ultrasound study (of 60 patients) by Han et al. (4) showed that when a single vein was present, it ran medially to the artery without exception. Such a disparity may originate from the limitations of the imaging techniques used in those studies: in the study by Glassberg et al. (3), 10-mm-thick CT scans were obtained, which were reviewed between the aortic arch and the main pulmonary artery; ultrasound was used in the study by Han et al. (4), a modality with a limited field of view and inability to visualize the post-chondral segments of the vessels. Besides, the study by Han et al. evaluated only the 2nd, 3rd, and 4th intercostal spaces (ultrasound) or 12 cm caudal to the sternomanubrial junction or below (CT), not giving information regarding courses of more cephalic portions of the IMs. In our case, the ability of MDCT to offer thin-section images, isotropic multiplanar reformations, and maximal intensity projections helped us to identify the unusual location of the IMV and trace the IMs through their entire courses.
The first of our cases, the anatomy of the IMs corresponded to the Arnez type 3, although the cadaveric study by those authors did not show how the IMA and IMV cross over around the first-rib level to join their respective innominate vessels. The patient was referred for transthoracic biopsy of a large anterior mediastinal mass, and there were wide windows for needle passages both medial and lateral to the internal mammary vessels. When planning a biopsy of a smaller mass in a similar location, the distance between the planned needle path and the internal mammary vessels can be shorter, and the operator may have to weigh the risk of the parasternal approach against that of the lateral approach. It has been emphasized to avoid both the IMA and IMV during a percutaneous procedure (3, 4), and there have been many reports of fatal hemorrhages from the IMA during both percutaneous and surgical procedures (1, 5-8). However, the literature is silent on the actual occurrence of a serious complication associated with IMV injury. Although we have successfully avoided both IMs during transthoracic biopsies so far, it is hard to understand how transgression of the IMV can possibly result in a massive hemorrhage, when much larger veins such as the brachiocephalic vein or the superior vena cava can be safely transgressed during needle biopsy (4, 9). Therefore, we believe that when a transthoracic biopsy path is set close to the IMs, it would be safe to choose the route away from the artery. Thus, we believe that pre-biopsy MDCT should be carefully reviewed to see whether the IMV is medial or lateral to the IMA. Usually, the IMV runs medially to the IMA in the first or second intercostals space, and it would be wise to plan a parasternal biopsy in such a patient. Nevertheless, when the IMV lies laterally to the IMA as in our first case, it may be safer to set the biopsy route laterally to the IMs unless there is enough distance between the sternal margin and the IMA.
In our second case, the IMV was found to cross over the IMA in the middle of the first intercostals space. To our knowledge, this particular pattern of IM course has never been reported in a cadaveric or imaging study. Although the parasternal route was not used in the biopsy of the second case, this case underscores the importance of careful review for IM course when preparing for a parasternal biopsy, which can be facilitated by the use of MDCT.
In summary, we present two cases in which the lateral location of the IMV and the medial location of the IMA were well-demonstrated for MDCT at the level of the first intercostals space. It is helpful to consider these variations in the IM course when planning and performing percutaneous biopsy with an anterior approach.


 XML Download
XML Download