

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Blunt thoracic trauma is a common reason for emergency room visits. Although the use of initial routine chest computed tomography (CT) is controversial, it is increasingly used for patients with traumatic injury, and has a higher diagnostic performance than that of plain radiographs (1-5).
Chest CT is useful for the evaluation of rib fractures. However, rib fractures can be missed by chest CT when there is no related change due to rib fracture and the fracture line is parallel to the CT section plane. The evaluation of ribs is particularly difficult due to their peripheral location. It is problematic for many radiologists when describing the fracture site in patients with rib fracture. Some clinicians use additional plain chest radiographs to overcome the limitations of CT in symptomatic patients; however, the patients are exposed to additional radiation during this process (6, 7). Three-dimensional reformation of the chest CT is helpful, but it takes more time for the radiologist to read the CT images (6, 8).
Recently, reformatting techniques have been used in many fields of radiology. These reformatting techniques make interpreting CT images more convenient and improve diagnostic performance because they provide additional information about the lesion (6, 9, 10). The reformatted images reflect the data with isotropic voxel and do not require additional radiation.
The purpose of our study was to assess the value of adding a reformatted CT rib series to transversely reconstructed CT images for the evaluation of rib fractures in patients with suspected traumatic thoracic injuries.
MATERIALS AND METHODS
Patient Population
From November 2009 to January 2010, a total of 100 consecutive patients with suspected traumatic thoracic injuries underwent chest CT. The patients included 66 men and 34 women, and the mean age was 54.7 years (age range from 15 to 93 years). Our retrospective evaluation of patient image data was approved by the local ethics committee.
CT Scanning
CT was performed using a 128-section multi-detector row CT scanner (Somatom Definition Flash; Siemens Medical Solutions, Forchheim, Germany). Patients were placed in the supine position on the table. A non-enhanced scan of the chest was acquired from the jugular fossa to the middle of the abdomen during an inspiratory breath hold. The detector configuration was 128 × 0.6 mm and the tube potential was 120 kVp. Automatic current modulation was used with CARE dose 4D (Siemens Medical Solutions, Erlangen, Germany). The gantry rotation speed was 0.5 s per rotation and the pitch was 1.1.
After performing the non-enhanced scan, an enhanced scan of the same region of the chest was acquired 80 seconds after an intravenous injection of nonionic contrast agent (1.8 mL/kg body weight, Pamiray 370; Iopamidol; Dongkook Pharm., Seoul, Korea). The non-enhanced and enhanced CT images were transversely reconstructed at 5-mm intervals and with 5-mm-thick slices. In addition, non-enhanced CT images with 0.6-mm-thick slices were reconstructed at 0.6-mm slice intervals, and were used to reformat the CT rib series.
Reformatting Technique
The reconstructed CT images were transferred to a three-dimensional (3D) workstation (Aquarius iNtuition; TeraRecon, Inc., San Mateo, CA, USA). Volume-rendered images were reformatted and reformatted data was affected by the gradient effect. Linear ramp-up with a window width of 400 Hounsfield units, a window center of 350 Hounsfield units, and 0.08 opacity were used for the gradient effect. According to this graph, the reformatted volume-rendered color image was converted to a black-and-white image with a gray-scaled gradient, similar to a plain radiograph (Fig. 1). The anteroposterior, sternal lateral, and oblique views were then captured. The images obtained by reformatting were similar to a rib series. These reformatted images were termed the "reformatted CT rib series." All of these processes were performed by one observer (S. N. M.) who was blinded to the purpose of this study.
Imaging Analysis
Three independent observers (S. K. J., with 23 years of experience in radiology; S. H. P., with 12 years of experience in radiology; and D. H. B., with 4 years of experience in radiology) retrospectively reviewed the images and were blinded to patient information and any other imaging results. The only patient information was provided from the patient's hospital number. Image reading occurred in 2 sessions. To reduce recall bias, the sessions were separated by a 4-week interval. During the first session, the 3 observers interpreted only the transverse CT images in separate rooms. During the second session, the observers interpreted each transverse image along with the reformatted CT rib series in separate rooms. For the second session, the 3 observers were provided a rearranged patient list, assembled by another radiologist S. N. M., which blinded the 3 observers to reduce recall bias. The recorded findings were classified by each patient and summarized. Together, the 3 observers then interpreted the 3D reformatted images generated by the 3D workstation and confirmed rib fractures by consensus.
Imaging findings included rib fracture and other injuries (hemothorax, pneumothorax, hydrothorax, parenchymal injury, chest wall swelling, intramuscular hematoma, aortic injury, mediastinal hematoma, airway injury, and abdominal visceral organ injury). A confidence score was obtained for each rib fracture, on a scale of 1-5 (1, definitely absent; 2, probably absent; 3, cannot determine; 4, probably present; and 5, definitely present).
Statistical Analysis
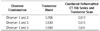
Receiver operating characteristic (ROC) curve analysis was used to estimate the diagnostic performance of each observer and the area under the ROC curve (Az) was calculated. To compare the diagnostic performance between the 2 sessions, pairwise comparisons of the ROC curves were performed and 95% confidence intervals were used to express the statistical precision of the results.
Based on the assumption that a confidence level of 4 or greater was positive for the diagnosis of rib fracture, diagnostic sensitivity, specificity, positive predictive value, and negative predictive value were calculated for the 3 observers and the McNemar test was used to compare sensitivity and specificity between the 2 sessions.
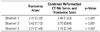
At each session, interobserver agreement was determined using the weighted κ statistic. A κ value of less than 0.20 indicated poor agreement, 0.21-0.40 indicated fair agreement, 0.41-0.60 indicated moderate agreement, 0.61-0.80 indicated good agreement, and greater than 0.81 indicated an excellent agreement.
Differences in the mean confidence ratings of each observer for patients with or without rib fractures were determined by the Wilcoxon signed rank test. p-values less than 0.05 were considered to indicate statistically significant differences. Statistics were calculated using SPSS 18.0 statistical software for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
We found 153 rib fractures in 29 out of 100 patients with suspected thoracic trauma. The area under the ROC curve improved for each observer when comparing the first and second session. Observer 1 improved from 0.918 to 0.960 (p < 0.001), observer 2 from 0.823 to 0.937 (p < 0.001), and observer 3 from 0.725 to 0.834 (p < 0.001) (Table 1). The diagnostic sensitivity of the 3 reviewers significantly improved in the second session (p < 0.001). The diagnostic specificity of observers 2 and 3 significantly improved in the second session (p = 0.012 for observer 2; p = 0.013 for observer 3) (Table 1). Interobserver agreement also improved in the second session (Table 2). The mean confidence scores of all observers for patients with rib fractures improved significantly in the second session (Table 3). The mean confidence scores of 2 observers (observer 1 and 3) for patients without rib fractures significantly improved in the second session, but that of the other observer (observer 2) did not improve significantly (Table 4).
DISCUSSION
In general, a rib fracture is considered a minor problem that only requires conservative therapy. However, rib fractures can cause serious conditions (11-13). It is difficult to detect rib fractures using transverse CT imaging alone, particularly if the related change is not combined and the fracture line is parallel to the slice plane.
To overcome this limitation of transverse CT images, slice thickness and intervals thinner than 5 mm, or 3D evaluation of chest CT data can be used. In the reformatted CT images, coronal, and sagittal image resolution is similar that of the transverse images. However, it takes a great deal of time for a radiologist to read. In contrast, a plain radiographic rib series can also be used. However, more radiation is required to obtain the images. Therefore, we found another method to detect rib fractures without the additional radiation dosage.
When we added a reformatted CT rib series to the transverse CT images, the following scores increased: sensitivity, interobserver agreement, and mean confidence. This suggests that the reformatted CT rib series allows for easier detection of rib fractures. In addition, for radiologists with less experience, their diagnostic performance can be improved using the reformatted CT rib series, compared to transverse CT images alone. In addition, although we did not measure reading time, interpretation using the reformatted CT rib series supports easier identification of the fractured rib site than using the transverse CT image alone.
The reformatted CT rib series was called a reformatted CT rib series; however, it is not same as a conventional rib series. Both images are 2 dimensional. The reformatted CT rib series was reformatted chest CT images, and their attenuation does not differ according to the distance from the tube. However, a conventional rib series is obtained by projection of an X-ray with one direction, and their attenuation differs according to the distance from the tube. In our study, stepladder artifacts mimicking rib fractures were rare because of the fast acquisition of CT scanning. Furthermore, this artifact can be differentiated from true fractures by noting their bilaterality and the continuing line abutting the fracture line.
Our study has some limitations. First, our study group was relatively small; however, there were 2400 ribs in our 100 patients. Second, only 3 radiologists participated in our study. Two of the reviewers were professors with more than 10 years of experience in radiology, and the other reviewer was a resident with 4 years of experience in radiology. Although they had different detection abilities, these differences were not statistically significant. Third, interpretation time was not recorded in this study. Therefore, we do not know exactly how much time was saved using the reformatted CT rib series compared to the 3D assessment of thoracic fractures. However, the interpretation time might be shorter when a reformatted CT rib series was added, because only 4 images were included in the series. In addition, we did not need to count the fractured rib. Finally, 3D thoracic assessment was used as the standard method for diagnosis of a thoracic fracture. Confirmation of thoracic fracture can be helped by a follow-up chest CT or bone scan. Although these examinations were not performed, some reports have shown that the 3D evaluation can improve diagnostic performance (14).
In conclusion, when compared to the use of a transverse CT scan only, the addition of a reformatted CT rib series was useful for the evaluation of patients with suspected traumatic injuries.



 XML Download
XML Download