

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Pancreatic panniculitis is an inflammation and necrosis of fat at distant foci in patients with pancreatic disorders, most frequently, pancreatitis and pancreatic carcinoma. Clinically, pancreatic panniculitis is manifested by painless or painful subcutaneous nodules on the legs, buttocks, or trunk. The usual sites are the distal parts of the lower extremities. To the best of our knowledge, there have not been many reports for the radiologic findings of pancreatic panniculitis. In this article, we report a case of pancreatic panniculitis, including radiologic findings of CT and ultrasonography. The patient was presented with painful subcutaneous nodules on the trunk, and had underlying acute pancreatitis and hemorrhagic pseudocysts.
Figures and Tables
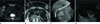
Fig. 1
32-year-old man with pancreatic panniculitis, associated with acute pancreatitis and hemorrhagic pseudocysts.
A. Precontrast axial CT scan shows large cystic mass (arrow) in the pancreatic head with peripancreatic infiltration. Focal area of high attenuation (asterisk) within the cystic mass suggests hemorrhage. Note the small subcutaneous nodule in the anterior abdominal wall (curved arrow).
B. Follow up abdomen CT after 3 days. Postcontrast axial CT scan shows multiple, mild enhancing nodules (arrows) with ill-defined margin and perinodular streaky densities in the anterior abdominal wall. Note focal area of low attenuation (arrowhead) indicating cystic portion of nodules.
C. Endoscopic retrograde cholangiopancreatography shows the irregular contrast filling of pancreatic pseudocyst (white arrow) communicating with the main pancreatic duct (black arrow).
D. Ultrasonography of abdominal subcutaneous nodule. The nodule is mainly cystic with some areas of echogenic solid portions (white arrow).
Note the increased vascularity within the solid portion and peripheral wall of nodule (asterisks).
References
1. Chiari H. Uber die sogenannte fettnekrose. Prager Med Wochenschr. 1883. 8:284–286.
2. Johnson MA, Kannan DG, Balachandar TG, Jeswanth S, Rajendran S, Surendran R. Acute septal panniculitis. A cutaneous marker of a very early stage of pancreatic panniculitis indicating acute pancreatitis. JOP. 2005. 6:334–338.
3. Echeverría CM, Fortunato LP, Stengel FM, Laurini J, Díaz C. Pancreatic panniculitis in a kidney transplant recipient. Int J Dermatol. 2001. 40:751–753.
4. Dhawan SS, Jimenez-Acosta F, Poppiti RJ Jr, Barkin JS. Subcutaneous fat necrosis associated with pancreatitis: histochemical and electron microscopic findings. Am J Gastroenterol. 1990. 85:1025–1028.
5. Berman B, Conteas C, Smith B, Leong S, Hornbeck L 3rd. Fatal pancreatitis presenting with subcutaneous fat necrosis. Evidence that lipase and amylase alone do not induce lipocyte necrosis. J Am Acad Dermatol. 1987. 17(2 Pt 2):359–364.
6. Trapp RG, Breuer RI, Crampton AR, Davis JH, Derman RE, Larson RH, et al. Pancreatic duct arteriovenous fistula and the metastatic fat necrosis syndrome. Dig Dis Sci. 1979. 24:403–408.
7. Mourad FH, Hannoush HM, Bahlawan M, Uthman I, Uthman S. Panniculitis and arthritis as the presenting manifestation of chronic pancreatitis. J Clin Gastroenterol. 2001. 32:259–261.
8. Szymanski FJ, Bluefarb SM. Nodular fat necrosis and pancreatic diseases. Arch Dermatol. 1961. 83:224–229.
9. Requena L, Sánchez Yus E. Panniculitis. Part II. Mostly lobular panniculitis. J Am Acad Dermatol. 2001. 45:325–361. quiz 362-364.
 XML Download
XML Download