

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Gynecologic disorders that cause pelvic pain in adolescents include hemorrhagic ovarian cysts, rupture or torsion of ovarian cyst or tumors, hematocolpos caused by vaginal obstruction, endometriosis, cystic uterine adenomyosis, pelvic inflammatory diseases, and pelvic inclusion cyst. The use of CT for the evaluation of pelvic pain is increasing, and CT is useful if ultrasound findings are not decisive and the lesion is extensive.
Figures and Tables
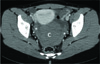
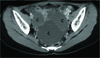
 | Fig. 1Hemorrhagic ovarian cyst in a 13-year-old girl who complained of abdominal pain in right lower quadrant area for one day. Precontrast axial scan shows a cystic mass with a fluid-fluid level (arrow) in right adnexa.
|
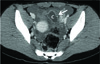
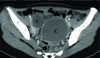
 | Fig. 2Hemorrhagic ovarian cyst in a 18-year-old girl who presented lower abdominal pain for one day. Precontrast axial scan shows a high attenuation cystic mass (C) in pelvic cavity. Also note high attenuation fluid collection in pelvic cavity (*), suggesting hemoperitoneum. It was proven as ruptured corpus luteal cyst of right ovary pathologically.
|
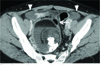
 | Fig. 3Rupture of hemorrhagic ovarian cyst in a 13-year-old girl who represented lower abdominal pain with rebound tenderness for 2 days. Postcontrast axial scan shows a irregular shaped cystic mass (C) with wall enhancement in pelvic cavity. An interruption of enhancing wall (arrow) is suggestive of rupture. Also note fluid collection in pelvic cavity. She was improved by the conservative treatment.
|
 | Fig. 4Rupture of ovarian dermoid cyst in a 15-year-old girl who complained of lower abdominal pain with tenderness and rebound tenderness. Postcontrast axial scan shows dermoid cyst with fat-fluid level and calcification, and fat (arrow) outside the tumor is identical to intratumoral fat. There is moderate amount of pelvic free fluid (arrowheads).
|
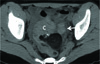 | Fig. 5Torsion of ovarian dermoid cyst in a 13-year-old girl who had lower abdominal pain with tenderness and rebound tenderness for three days. Precontrast axial scan shows a high attenuation mass (C) with fat and calcification containing cystic mass, suggesting torsion of underlying ovarian dermoid cyst. A high attenuation nodular lesion (arrow) adjacent to cystic mass is suggestive of tubal hemorrhage.
|
 | Fig. 6Ovarian torsion in a 14-year-old girl who complained of nausea and abdominal pain in right lower quadrant area for two days.
A. Precontrast axial scan shows high attenuation mass (C) with cystic component in pelvic cavity.
B. Postcontrast axial scan shows that left ovary (arrow) is normal in position and uterus is deviated to right side. Salpingoophorectomy was done, and it was diagnosed as hemorrhagic infarction of right ovary pathologically.
|
 | Fig. 7Ovarian torsion with hematosalpinx in a 11-year-old girl.
A, B. Postcontrast axial scans show large low attenuation mass-like lesion (arrowheads) with small cystic lesion (arrows) in anterior portion of lower abdominal and pelvic cavity, suggesting torsed left ovary. Uterus is deviated to left side. A large cystic mass (C) with wall enhancement is in pelvic cavity. It was diagnosed as left ovarian torsion and hematosalpinx surgically, so detorsion of twisted left ovary and cystectomy of left adnexa were done. The cystic lesion was confirmed as hemorrhagic necrosis of fallopian tube pathologically.
|
 | Fig. 8Ovarian torsion in a 10-year-old girl who complained of fever and low abdominal pain for four days.
A, B. Postcontrast axial scans show enhancing soft tissue mass-like lesion (arrowheads) connecting to torsed enlarged left ovary (O). It represents a twisted thickened fallopian tube. Detorsion of left adnexal torsion was done.
|
 | Fig. 9Torsion of paratubal cyst in a 14-year-old girl who had lower abdominal pain with tenderness and rebound tenderness for three days.
A. Transabdominal ultrasonography shows echogenic mass (M) near normal right ovary (arrow).
B. Postcontrast axial CT scan shows normal ovary (arrow) and cystic mass (M) in right adnexa. It was confirmed by torsion of paratubal cyst at surgery.
|
 | Fig. 10Didelphic uterus and obstructed hemivagina-ipsilateral renal agenesis anomaly in a 18-year-old girl who presented with abdominal pain and tenderness in right lower quadrant pain for one day.
A, B. Postcontrast axial (A) and coronal (B) images show multiple cystic and tubular structures (arrowheads) with enhancing wall in right lower quadrant abdomen, suggesting hematosalpinx. Also note didelphic uterus (U) and fluid collection in dilated right hemiuterus and dilated right hemivagina (V) on coronal image (B).
|
 | Fig. 11Transvaginal septum in a 10-year-old girl who presented as lower abdominal pain and hypermenorrhea.
A. Postcontrast axial scan shows fluid collection in uterine cavity (U) and vagina (V).
B, C. Postcontrast coronal (B) and sagittal (C) images shows thin horizontal septum (arrow) in the midportion of dilated vagina (V). Also note fluid collection in endometrial cavity (arrowhead). On coronal image, right kidney is absent.
|
 | Fig. 12Hematocolpos caused by imperforate hymen in a 14-year-old girl. She had lower abdominal pain for two weeks, and abdominal pain was progressed.
A. Postcontrast sagittal image shows fluid collection in markedly dilated vagina (V) and slightly dilated endometrial cavity.
B. Precontrast axial scan shows high attenuation fluid collection in dilated vagina (V) and high attenuation fluid in right anterior pelvic cavity (arrowhead). It was confirmed as hemoperitoneum by endometriosis at laparoscopic biopsy.
|
 | Fig. 13Hematometrocolpos of double vagina caused by imperforate hymen associated with longitudinal vaginal septum and uterine didelphys. A 13-year-old girl presented with lower abdominal pain for 2 days. Oblique coronal postcontrast image shows markedly distended vagina. A longitudinal septum (open arrowheads) splits the vagina into two compartments.
|
 | Fig. 14Endometriomas in a 19-year-old girl. Postcontrast axial scan shows multiple cystic lesions (C) of both ovaries with "kissing ovary sign".
|
 | Fig. 15Endometriomas in a 19-year-old girl. She complained of lower abdominal pain and fever for 10 days, and she had severe dysmenorrhea. Postcontrast axial scan shows two thin walled cystic masses (C) in pelvic cavity. Bilaterality and multiple lesions supported the diagnosis of endometriosis rather than hemorrhagic ovarian cyst.
|
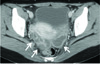
 | Fig. 16Cystic uterine adenomyosis in a 14-year-old girl who presented with lower abdominal pain for two days. She had also presented with severe dysmenorrhea.
A. Precontrast axial scan shows low attenuation mass (arrow) in uterine myometrium.
B. Postcontrast sagittal image shows low attenuation mass (arrow) with irregular enhanced wall in uterine myometrium.
|
 | Fig. 17Bilateral pyosalpinx in a 19-year-old girl. Postcontrast axial scan shows dilated thickened enhancing fallopian tubes (arrows) containing fluid, suggesting pyosalpinx.
|
 | Fig. 18Pelvic inclusion cyst in a 15-year-old girl. She had the history of operation of ileal atresia at neonatal period. Ileoileal anastomosis was also done due to foreign body lodging at the anastomotic site when she was 8 years old. At that time, there was no fluid collection in abdominal and pelvic cavity on abdominal CT.
A, B. Postcontrast axial (A) and coronal (B) images show irregular shaped fluid collection in right lower abdominal and pelvic cavity, conforming to the borders of adjacent organs or the peritoneal wall. A normal-appearing ovary (arrow) is surrounded by loculated fluid. At pathologic examination, mesothelial cells were lined on some portion of cystic wall.
|
References
1. Garel L, Dubois J, Grignon A, Filiatrault D, Van Vliet G. US of the pediatric female pelvis: a clinical perspective. Radiographics. 2001; 21:1393–1407.
2. Potter AW, Chandrasekhar CA. US and CT evaluation of acute pelvic pain of gynecologic origin in nonpregnant premenopausal patients. Radiographics. 2008; 28:1645–1659.
3. Bennett GL, Slywotzky CM, Giovanniello G. Gynecologic causes of acute pelvic pain: spectrum of CT findings. Radiographics. 2002; 22:785–801.
4. Choi HJ, Kim SH, Kim SH, Kim HC, Park CM, Lee HJ, et al. Ruptured corpus luteal cyst: CT findings. Korean J Radiol. 2003; 4:42–45.
5. Rha SE, Byun JY, Jung SE, Jung JI, Choi BG, Kim BS, et al. CT and MR imaging features of adnexal torsion. Radiographics. 2002; 22:283–294.
6. Stark JE, Siegel MJ. Ovarian torsion in prepubertal and pubertal girls: sonographic findings. AJR Am J Roentgenol. 1994; 163:1479–1482.
7. Okada T, Yoshida H, Matsunaga T, Kouchi K, Ohtsuka Y, Takano H, et al. Paraovarian cyst with torsion in children. J Pediatr Surg. 2002; 37:937–940.
8. Junqueira BL, Allen LM, Spitzer RF, Lucco KL, Babyn PS, Doria AS. Müllerian duct anomalies and mimics in children and adolescents: correlative intraoperative assessment with clinical imaging. Radiographics. 2009; 29:1085–1103.
9. Emmert C, Romann D, Riedel HH. Endometriosis diagnosed by laparoscopy in adolescent girls. Arch Gynecol Obstet. 1998; 261:89–93.
10. Ho ML, Raptis C, Hulett R, McAlister WH, Moran K, Bhalla S. Adenomyotic cyst of the uterus in an adolescent. Pediatr Radiol. 2008; 38:1239–1242.
 XML Download
XML Download