

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Endoscopic thyroidectomy has recently been used for the treatment of benign nodules and thyroid cancer (1). The use of endoscopic thyroidectomy is increasing because of the increased prevalence of micropapillary carcinoma and a significant number of patients comprising of young women look for the treatment option that provides a better cosmetic result (2). In Asia, Ohgami et al. (3) first proposed and performed extracervical approaches for endoscopic thyroidectomy using an "anterior chest wall" and a "scarless" breast approaches. More recently, various endoscopic thyroid surgery techniques have been developed. Many groups from Asia have focused on endoscopic thyroidectomy via axillary approaches (45). Other groups have since described an axillo-breast approach (1678). At our institution, endoscopic thyroidectomy via unilateral and bilateral axillo-breast approaches is used (17).
After surgical treatment, patients with thyroid cancer are monitored closely for recurrence using various methods including physical examination, ultrasonography (US), iodine-131 whole-body scanning, and tumor markers such as thyroglobulin (Tg) and Tg antibody. US gives the highest sensitivity among these methods (91011). More recently, the technique of analyzing fine-needle aspiration specimens for Tg has been added as a reliable index for the diagnosis of recurrence (10121314).
These assessments for the detection of recurrence are the same in conventional and endoscopic thyroidectomy. In a postoperative clinical follow-up of patients who underwent endoscopic thyroidectomy, we encountered 13 foreign body granulomas in the surgical bed. Subsequently, US findings of the foreign body granulomas were retrospectively evaluated for characteristic US findings.
Identifying the characteristic US findings of foreign body granulomas is important because it raises concerns about recurrence; thus, unnecessary imaging modalities and invasive procedures can be avoided and tumor recurrence and other pathologic conditions can be excluded.
The purpose of this study was to assess the US findings of foreign body granulomas in the surgical bed after endoscopic thyroidectomy via an axillo-breast approach.
MATERIALS AND METHODS
Study Population
The institutional review board approved the present retrospective study and informed consent was waived. During the period January 2007 to June 2011, 268 cases of unilateral or total endoscopic thyroidectomy were performed at the Department of Otolaryngology-Head and Neck Surgery at our hospital. In the postoperative clinical follow-up of patients who underwent endoscopic thyroidectomy, we encountered two patients complaining of palpable lesions in the anterior chest wall. We performed positron emission tomography-computed tomography (PET-CT) with concern regarding Recurrence or seeded tumor. The lesions showed increased fluorodeoxyglucose (FDG) uptake on PET-CT scanning. Diagnostic US was performed and lesions were confirmed to be foreign body granulomas by gun biopsy. PET-CT scan of another patient showed a lesion in the surgical bed that showed increased FDG uptake. The lesion was confirmed to be foreign body granuloma by fine needle aspiration biopsy. Next, we included chest wall scanning in the follow-up US of patients who underwent endoscopic thyroidectomy. Subsequently, 11 additional lesions that demonstrated US findings similar to biopsy-proven foreign body granulomas were detected in 10 other patients who underwent endoscopic thyroidectomy. A patient with a lesion whose underlying pathologic diagnosis was papillary thyroid carcinoma was excluded from the study because it has no follow-up US or CT scan. Other 9 patients were clinically diagnosed by characteristic US findings and serum Tg and Tg antibody levels. Finally, three pathologically proven lesions and 10 additional lesions - a total of 13 lesions from 12 patients (three men and nine women; mean age, 38 years; age range, 27-55 years) - were included in the current retrospective study. Serum Tg and Tg antibody levels of four patients who underwent total or completion thyroidectomy were assessed at the time of follow-up US (same day as US in 3 patients, 10 days prior in 1 patient). The pathologic diagnosis of the underlying lesions of eight patients was papillary thyroid carcinoma (seven of eight were microcarcinomas) and that of the other three patients was nodular hyperplasia.
Endoscopic Thyroidectomy
Ten patients underwent endoscopic hemithyroidectomy and two patients had endoscopic total thyroidectomy. Two of ten patients who underwent endoscopic hemithyroidectomy had undergone completion thyroidectomy due to papillary thyroid cancer with lymph node metastasis.
Surgery was performed as follows: a 4.5- to 5.5-cm skin incision was made parallel to the skin crease in the axillary fossa, into which the rigid endoscope and endoscopic instruments were inserted. The skin was elevated above the pectoralis major muscle exclusively under direct vision using monopolar cauterization through the axillary skin incision until the anterior border of the sternocleidomastoid muscle was exposed. A second 1.0-cm skin incision was made along the upper margin of the mammary areola on the tumor side for the insertion of a 12-mm trocar, which was directed to the midline of the sternal notch. The anterior border of the sternocleidomastoid muscle was dissected from the sternohyoid muscle, and in some cases, divided the omohyoid muscle. In all cases, only the harmonic scalpel (HS; Harmonic Ace 36P®; Johnson & Johnson Medical, Cincinnati, OH, USA) was used for the vascular control of the thyroid gland and strap muscles (17).
US and Other Imaging Studies
US was performed using an IU22 US, an HDI 5000 with an L12-5 (5-12 MHz) linear array transducer (Philips Medical Systems, Bothell, WA, USA), a LOGIQ 700 MR with an LA39 (6-13 MHz) linear array transducer, and a LOGIQ E9 system with an ML6-15-D (5-16 MHz) linear array transducer (GE Healthcare, Milwaukee, WI, USA). A head and neck radiologist with 20 years of experience in thyroid sonography scanned all the patients and reviewed the US findings for lesion echogenicity, shape and size. Color Doppler US was available in 11 lesions, and the presence or absence of vascular flow signals within the lesions was assessed. No evaluation was performed on the flow patterns in the other two lesions. The color gain was adjusted until the background noise first became apparent. US-guided gun biopsy was performed on two lesions using a needle biopsy gun (Acecut; TSK Laboratory, Tochigi, Japan) with an 18-gauge × 7.5-cm needle and a 22-mm biopsy specimen notch. Fine needle aspiration biopsy was performed on one lesion with a 22-gauge needle attached to a 10-mL plastic syringe, using a freehand technique. The mean time from thyroidectomy to lesion detection on US was 481 days (range, 182-815 days). Eleven lesions underwent follow-up US for an evaluation of evolutional change over time. The mean interval time from lesion detection to follow-up US was 275 days (range, 45-494 days). The time of the first US after endoscopic thyroidectomy was varied because it depended on multiple factors including the type of underlying lesion, presence of symptoms, abnormal laboratory findings and clinical follow-up loss. Ten of 13 lesions were detected on the first US after surgery. However, two other lesions (lesion no. 9 and no. 10) were detected on the second US; we believed that we missed the lesions on the first US because the lesions were ill-defined and isoechoic compared with the adjacent muscle at the time of the first US. Additionally, the other lesion (lesion no. 11) was detected on the fourth US because the lesion was located in the anterior chest wall and three previous US scans did not include the chest wall. Two lesions did not undergo follow-up US. One lesion had been followed up by contrast enhanced neck CT after 625 days from the initial US and showed no evidence of recurrence or seeded neoplasm. Another lesion did not require clinical follow-up because the underlying pathology was determined as nodular hyperplasia.
Furthermore, four lesions were evaluated by CT, three by PET-CT, and one by both CT [(n = 3; LightSpeed VCT; GE Healthcare) and (n = 1; Somatom Sensation 16; Siemens Medical Solutions, Erlangen, Germany)] and PET-CT (Biograph2 scanner; Siemens Medical Systems, Forchheim, Germany).
Statistical Analysis
Foreign body granulomas were divided into two groups based on the echogenicity and the shape of the lesions (group I: hyperechoic linear lesions with posterior acoustic shadowing, n = 7; group II: oval lesions, iso- to slightly hypoechoic relative to the adjacent strap muscle or the pectoralis major muscle, n = 6). The time from thyroidectomy to lesion detection was compared between the two groups using the Mann-Whitney test. The relationship between the largest diameter of the lesion and the time from thyroidectomy to lesion detection was examined using Spearman's correlation coefficient. Nonparametric tests were applied to ensure that small sample sizes were properly handled. A p-value less than 0.05 was deemed to indicate a statistically significant difference. Statistical analysis was performed using Stata 11 software (Stata, College Station, TX, USA).
RESULTS
Clinical and US findings are summarized in Table 1.
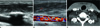
The mean serum Tg level of four patients who had undergone a total or completion thyroidectomy was 0.30 ng (range, 0.01-1.02 ng). Additionally, the mean serum Tg antibody level of those four patients was 0.10 ng (range, 0.01-0.37 ng). On US, seven lesions were curved or straight hyperechoic linear lesions with posterior acoustic shadowing (Figs. 1A, 3A); six other lesions were oval and well-defined masses, which were isoechoic (n = 3) (Fig. 2A) or slightly hypoechoic (n = 3) relative to the adjacent muscle. The lesions were located in the anterior chest wall (n = 6), sternocleidomastoid muscle (n = 4), and strap muscle (n = 3).
Color Doppler US in 11 lesions revealed no blood flow (Figs. 1B, 2B, 3B). Color Doppler US was not available in the other two lesions. The mean largest diameter of the lesions was 17 mm (range, 10-20 mm). The size of the lesions was inversely correlated with the time to lesion detection (Spearman's correlation r = -0.6528; p < 0.02). Thus, we could presume that the lesions had decreased in size over time. The mean time from thyroidectomy to lesion detection on US was 318 days for hyperechoic lesions and 672 days for solid lesions. Solid lesions had a significantly longer time to lesion detection than hyperechoic lesions (Mann-Whitney test, p = 0.01).
Histopathology showed a foreign body granuloma with multiple empty spaces and remnant amorphous material in a case with a hyperechoic linear lesion with posterior acoustic shadowing on US (Fig. 1E). A well-defined, oval iso- to slightly hypoechoic solid lesion without posterior acoustic shadowing on
US revealed a foreign body granuloma with denser fibrosis and only a few empty spaces (Fig. 2E). On follow-up US, hyperechoic linear lesions (n = 6) with posterior acoustic shadowing showed either a decrease in size only (n = 4) or became oval, iso- to slightly hypoechoic lesions with a decrease in size (n = 2) (Figs. 1B, 3B). Evolutional change of the oval, iso- to slightly hypoechoic lesions (n = 5) was disappearance (n = 3) and decrease in size (n = 2). One lesion followed up by contrast enhanced neck CT without follow-up US (No. 2) showed a decrease in size.
Discussion
Neck US is performed as the first-line imaging modality in the follow-up of patients with postoperative thyroid cancer (10). On US, the normal postoperative thyroid bed should have a uniform echogenic texture owing to the fibrofatty connective tissue (15). Any hypoechoic mass detected in the postoperative thyroid bed on US is suggestive of recurrence, in which case a biopsy should be performed. Even a well-differentiated papillary thyroid carcinoma is reported to be associated with a significantly increased rate of thyroid cancer mortality (1617). However, several benign pathologies mimicking tumor recurrence in the thyroid bed exist including thyroid remnants, postoperative scars, suture granulomas, chronic granulomatous lesions, muscletissue and fat necrosis (1819202122).
Incidental reports have been published regarding recurrences at the site of insertion of the laparoscopic instruments in various cancers. One case report described a 25-year-old woman who had recurrent cancers around the operative bed and subcutaneous tunnel after endoscopic thyroidectomy (23). Needle tract implantation of thyroid carcinoma after fine-needle aspiration has been occasionally reported (24). Another report described soft tissue implantation of thyroid adenomatous hyperplasia after endoscopic thyroidectomy (25). According to a review, multiple factors - including the gas used, local trauma, tumor manipulation, biologic properties of the tumor, and individual surgical skills - were associated with recurrence in the surgical bed (26).
Kamaya et al. (27) reported that thyroidectomy bed recurrence possesses characteristic sonographic features including hypoechoic echogenicity compared with the adjacent fibrofatty tissue, detectable internal vascularity on color Doppler or power Doppler imaging, and lesions that may or may not contain microcalcifications or coarse calcifications. They reported 100% detectable vascularity in recurrent malignancies. Conversely, Shin et al. (22) concluded that they could not differentiate benign tissues from recurrences by US without fine-needle aspiration. They reported that 70% of their lesions to be hypoechoic and the remaining 30% to be markedly hypoechoic. They also examined vascularity and 65% of their recurrences were examined using color Doppler US; however, only 23% of the recurrent lesions were vascular. Although controversy exists regarding the vascularity of recurrence, no foreign body granuloma in our study showed vascularity. The mean largest diameter of foreign body granulomas in the current study was 17 mm (range, 10-20 mm). Recurrent tumors with such large sizes may demonstrate vascularity on color Doppler US.
A suture granuloma is a benign, granulomatous inflammatory lesion characterized by a histiocytic reaction with foreign body giant cells around nonabsorbable sutures. Suture granulomas can also be found in the thyroid bed after thyroidectomy and mimic recurrent thyroid tumors (18). However, in endoscopic thyroidectomy via the axillo-breast approach used at our institution, a harmonic scalpel without suture material is employed for hemostasis; thus, suture granuloma can be excluded. Kim et al. (18) concluded that the typical US features of suture granulomas are those of ill-defined, heterogeneous and irregular hypo- to isoechoic lesions, with multiple central or paracentral internal echogenic foci > 1 mm. In their study, 9 of 10 suture granulomas disappeared or decreased in size during follow-up. This feature of disappearing or decreasing size is the consistent with the findings in foreign body granulomas after endoscopic thyroidectomy in the present study. Thus, we suggest that if a lesion exists with suspicious findings of foreign body granulomas, follow-up US may be useful to exclude recurrence without having to perform biopsy.
Langer et al. (20) reported four cases of chronic granulomatous lesions after thyroidectomy and concluded that the diagnosis may be suggested when the lesion shows the US appearance of a poorly defined, hypoechoic lesion with a central echogenic non-shadowing focus. The US features of those lesions were similar to that of a suture granuloma. However, in their study, no evidence was found of a suture or other foreign body in the only patient who had surgical excision. Additionally, those lesions appeared as complex cystic masses on CT and magnetic resonance imaging, and had increased activity on PET.
Suture granulomas (18) and chronic granulomatous lesions (20) after thyroidectomy have been reported. However, US and CT findings of suture granulomas and chronic granulomatous lesions were different from those of foreign body granulomas in the present study, and the technique of endoscopic thyroidectomy performed at our institution does not use suture material (151819202122). Foreign body granulomas, excluding suture granulomas and chronic granulomatous lesions, after endoscopic thyroidectomy or conventional thyroidectomy have not been previously reported. Additionally, lesions of characteristic US findings of foreign body granulomas have not been observed in the follow-up US of patients who had conventional thyroidectomy. Thus, we presumed that US findings of these foreign body granulomas are related to the endoscopic approach of thyroidectomy.
Our study found characteristic sonographic findings and its evolutional change. On early US, foreign body granulomas showed hyperechoic linear lesions with posterior acoustic shadowing, but without vascularity on color Doppler images. Over time, these granulomas decreased in size and changed into well-defined oval iso- to slightly hypoechoic lesions. Ultimately, these granulomas disappeared.
Hyperechogenicity with posterior acoustic shadowing on US revealed a foreign body granuloma with multiple empty spaces on pathology. We presumed that the reflection of the US beam between the empty spaces produced these US findings. A well-defined, oval iso- to slightly hypoechoic lesion without posterior acoustic shadowing on US showed denser fibrosis and very few empty spaces on microscopic examination. These different microscopic findings are correlated with the evolutionary changes in the foreign body granuloma.
The CT findings of several suture granulomas of other organs have been reported (28293031). Ferrozzi et al. (28) reported a case of foreign body granuloma of the kidney that was a well-capsulated renal mass with intralesional calcifications and adipose foci without infiltration of the surrounding structures on CT. The lesion was confirmed by histologic examination as a nonspecific, chronic granulomatous inflammation secondary to a foreign body (suture material). Moreover, Kim et al. (30) reported two foreign body granulomas in the abdomen: one demonstrated an oval, well-defined, hypodense mass with peripheral contrast enhancement and the other revealed a well-enhancing mass. However, foreign body granulomas in our study demonstrated oval, well-defined nodular lesions iso- to slightly hyperdense compared to the adjacent muscle with enhancement on CT. These CT findings were different from those of the above suture granulomas.
Significantly increased 18F-fluorodeoxyglucose uptake in the neck of a patient who underwent thyroidectomy has been reported using combined PET and CT (32), which was found to be localized to the left vocal cord presumably because of a Teflon-induced granuloma. Foreign body and infectious granulomas are well known to demonstrate increased FDG uptake. Thus, foreign body granulomas are often difficult to differentiate from malignant lesions.
Foreign body granulomas in our study were located in the anterior chest wall (n = 6), sternocleidomastoid muscle (n = 4), and strap muscle (n = 3). The lesions in the anterior chest wall were in the superficial layer of the pectoralis major muscle. In the endoscopic thyroidectomy via the axillo-breast approach, the skin was elevated above the pectoralis major muscle until the anterior border of the sternocleidomastoid muscle was exposed. Additionally, a 12-mm trocar was directed to the midline of the sternal notch through the periareolar skin incision. The mean largest diameter of the foreign body granulomas in our study was 17 mm, similar to the size of the used trocar. Additionally, an external retractor and rigid endoscope were inserted and moved in the narrow operative space, and the anterior chest wall and lower neck could be pressed by these instruments. We presumed that this pressure effect produced by endoscopic instruments can also result in considerable irritation and foreign body reaction of the chest wall and lower neck tissue. In conclusion, we thought that these foreign body granulomas were related to the use of endoscopic instruments and hyaluronic acid (Guardix-sol®; Hanmi Medicare, Seoul, Korea) as an anti-adhesive barrier in endoscopic thyroidectomy.
Our study had several limitations. First, only 3 of 13 lesions were confirmed by pathology to be foreign body granulomas. The others were only clinically diagnosed by characteristic US findings and follow-up US. However, those lesions demonstrated evolutional changes, including decreased size and echogenicity, and the lesions showed similar US findings as pathologically confirmed lesions. Thus, invasive biopsy was not necessary. Additionally, the serum Tg levels of four patients who underwent total or completion thyroidectomy were < 2 ng/mL (mean, 0.3 ng/mL; range, 0.01-1.02 ng/mL), and the Tg antibody levels of those four patients were not significant (mean, 0.1025 ng/mL; range, 0.01-0.37 ng/mL). Therefore, we excluded the possibility of tumor recurrence for those five lesions of four patients. Additionally, lesions in the anterior chest wall are obviously unusual for recurrence considering their location and tumor seeding in the subcutaneous tunnel after endoscopic thyroidectomy is very rare. Thus, we could presume the possibility of nonrecurrent lesions for encountered lesions on US. However, a prospective study should be performed to establish characteristic imaging findings of foreign body granulomas after endoscopic thyroid-ectomy. The second limitation of the present study is that this was a retrospective study, thus findings on Doppler US and follow-up US were not available for all lesions. Also, the times of US studies were varied among patients.
In summary, foreign body granulomas after endoscopic thyroidectomy show hyperechoic linear lesions with posterior acoustic shadowing in the early phase and oval, iso- to slightly hypoechoic solid lesions in the later phase. These lesions show evolutional change over time from a decrease in size and echogenicity, to becoming a well-defined margin and finally disappearing. Although suspicious lesions in the thyroidectomy bed should be biopsied percutaneously for pathologic confirmation, if the lesions show characteristic US findings of foreign body granulomas, performance of invasive procedures is not necessary. Instead, follow-up US may be helpful for the diagnosis.



 XML Download
XML Download