

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bronchogenic cysts are congenital malformations thought to develop from abnormal budding of the tracheobronchial tree (1). In normal development, the tracheal bud arises from the embryonic foregut around the fourth week of gestation, and undergoes further branching. If abnormal budding occurs during this process, a blind-ended pouch lined with pseudostratified columnar respiratory epithelial cells develops and forms a bronchogenic cyst. The location of a bronchogenic cyst depends on when the abnormal budding occurred. The cysts are most commonly seen in the mediastinum, especially in the middle and the posterior mediastinum, and can be located in lung parenchyma. The attenuation value is dependent on the contents of the cyst. Although the name is bronchogenic 'cyst', the attenuation value can be more than 100 HU if the cyst contains a large amount of protein or calcium. Due to variability in location and internal density, it is often difficult to diagnose bronchogenic cysts on CT scan.
With this background, Cardinale et al. (2) proposed diagnostic criteria based on those two factors, the location and the CT density of the lesion. According to these criteria, if the mass was located in a typical location (the middle mediastinum) and showed typical attenuation (fluid attenuation, 0-20 HU), a diagnosis of bronchogenic cyst was considered. However, if the mass was located in an atypical location for bronchogenic cysts and showed soft-tissue attenuation, other diagnoses were considered.
In our study, we encountered 3 cases of anterior mediastinal well-circumscribed masses with soft-tissue attenuation. Because of their location and attenuation characteristics these lesions were diagnosed as thymoma preoperatively. However, they were later identified to be bronchogenic cysts on histopathology. As mentioned above, anterior mediastinal bronchogenic cysts are extremely rare. Furthermore, there have been a few cases of anterior mediastinal bronchogenic cysts showing water-attenuation and therefore mimicking thymic cysts that have been reported on previously (3). However, anterior mediastinal bronchogenic cysts with soft-tissue attenuation have not been reported in the English literature up until now. The cases in our study indicate the possibility of an anterior mediastinal location for bronchogenic cysts, and the potential for these cysts to show soft-tissue attenuation.
CASE REPORT
Case 1
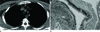
A 43-year-old male patient presented to our outpatient clinic with an incidentally-discovered mass in the anterior mediastium. His medical history was unremarkable except for a history of mitral valve insufficiency but no significant abnormality was noted on physical examination or in the laboratory tests. Chest radiography showed no abnormal finding except for bilateral pulmonary edema. Non-contrast enhanced chest CT scan (Fig. 1A) showed a well-circumscribed soft-tissue homogenously-attenuated (ROI = 35 HU, SD = 19.15) mass in the anterior mediastinum. Because the location and density of this mass were compatible with thymoma, this lesion was diagnosed as being a thymoma preoperatively, but it was later identified as a bronchogenic cyst on pathology (Fig. 1B).
Case 2
A 46-year-old female patient was admitted to our hospital 348with an incidentally-discovered anterior mediastinal mass. She did not complain of any symptoms, and there was no past history of illness. Chest radiography revealed no significant abnormality in the chest. Transverse pre-contrast enhanced CT scan (mediastinal window settings) (Fig. 2) showed a 3.2 cm well-circumscribed soft-tissue attenuated (ROI = 25 HU, SD = 3.91) lesion in the anterior mediastinum. This lesion showed homogenous internal attenuation which was less than that of soft tissue such as chest wall muscle. After injection of contrast material, there was slight thin-wall enhancement. Internal enhancement was not seen. We tentatively diagnosed thymic cyst or thymoma based on the location and density of the lesion. However, on pathology, this lesion was confirmed to be a bronchogenic cyst.
Case 3
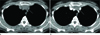
A 65-year-old female patient was admitted to our cardiology center with chest pain. EKG showed no significant abnormality, and serum cardiac enzymes were in the normal range. We could not detect any abnormality in the chest radiography. The cardiologist recommended a chest CT scan be performed. A transverse pre-contrast enhanced CT scan (mediastinal window settings) (Fig. 3A) showed a 2-cm well-circumscribed soft-tissue attenuated (ROI = 57 HU, SD = 45.60) lesion in the anterior mediastinum. This lesion showed homogenous attenuation similar to that of soft tissue. In contrast-enhanced CT scan (Fig. 3B), there was no enhancement of the lesion (57 HU → 47 HU). According to the classification proposed by Cardinale et al. (2), a diagnosis of bronchogenic cyst could not even be considered. Because it was thought to be a thymoma, the patient was operated on and the lesion was sent for pathologic examination (Fig. 3C, D), which showed that the lesion was a bronchogenic cyst.
DISCUSSION
Bronchogenic cysts are a congenital anomaly arising from abnormal budding of the ventral foregut, a development which occurs during the first 16 weeks of gestation (4). Instead of developing into a bronchus, the abnormal ventral bud differentiates into a fluid-filled blind-ended pouch (5). Bronchogenic cysts typically manifest as well-circumscribed non-enhancing middle mediastinal masses with water-attenuation. Despite bronchogenic cysts not being an uncommon finding, two factors cause radiologists to misdiagnose them. The first is the variable density of bronchogenic cysts, and the second is their variable location. We need to know the location of atypical sites and we need to know the full range of CT density of bronchogenic cysts, and diagnosis should take into account these two factors.
The fluid in the bronchogenic cysts contains water and protein, therefore bronchogenic cysts show a wide variation in CT-density according to the proportion of protein contained in the cyst (6). Although mediastinal bronchogenic cysts typically show a density that is similar to that of water, one study on CT attenuation in 58 pathologically-confirmed bronchogenic cysts revealed that 43% of cases showed soft-tissue attenuation (above 20 HU) (5). Because of this, bronchogenic cysts can mimick other masses, such as lymphomas or neurogenic tumors.
Bronchogenic cysts may occur in any part of the mediastinum (70-85%) (78). Other less common sites are lung parenchyma (15-30%) (57910), pleura and diaphragm (5). As mentioned above, bonchogenic cysts are typically located in the middle mediastinum, especially in the subcarinal area, and it is not rare to find them in the posterior mediastinum. However, only two cases of anterior mediastinal bronchogenic cysts have been reported in the English literature up until now (3). These anterior mediastinal bronchogenic cysts showed cystic attenuation so they were diagnosed as thymic cysts preoperatively.
Cardinale et al. (2) ENREF 3 have proposed diagnostic criteria based on the typical location and the typical CT density of bronchogenic cysts. They defined the typical location as being the subcarinal area and the typical density as water density (between 0-20 HU). If the lesion showed both typical findings, it was classified as Level 1, likely diagnosis. If the lesion displayed only one of the typical findings, it was classified as Level 2, possible diagnosis. If the lesion did not demonstrate any of the typical findings, it was classified as Level 3, unlikely diagnosis. In that study of 21 bronchogenic cysts, there was no cyst classified as Level 3.
In our study, all of the three anterior mediastinal lesions showed soft-tissue attenuation (above 20 HU). Under Cardinale's classification system, these lesions would have been classified as Level 3, unlikely diagnosis. Although contrast enhancement was not demonstrated in our cases, we misdiagnosed these lesions as thymoma due to their location and density. The cysts in our study are the first cases of anterior mediastinal bronchogenic cyst showing soft-tissue attenuation on imaging that have been reported in the medical literature.

 XML Download
XML Download