

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastric metastasis or carcinomatosis from primary breast cancer is a rare phenomenon. It is more prevalent in the invasive lobular type of breast cancer, although the most common histologic subtype of breast cancer is the invasive ductal type (1234). To date, there are only a few case reports demonstrating that gastric metastases were manifested as an initial presentation of invasive lobular breast cancer (56789). Nevertheless, most of the cases were distant recurrences occurring in patients with breast cancer histories (5678). As of now, there is only one published case study reporting about gastric metastasis originating from occult breast lobular cancer and its focus was mainly on the distinct immunohistochemical features between primary gastric cancer and metastatic breast cancer (9). Therefore, in our report of a case of invasive lobular breast cancer identified by gastric metastasis, its imaging features, which significantly contributed to the detection of occult breast cancer, were described.
CASE REPORT
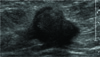
A 57-year-old woman was admitted to our institution with a chief complaint of general weakness and suspicion of gastric malignancy through an outside hospital. She had a non-specific clinical history. A physical examination had no obvious findings according to the medical records. Upper gastrointestinal endoscopy showed a huge depressed-ulcerative lesion covered with whitish exudate at the lower body to the antrum of the stomach. Subsequently, endoscopic biopsy was also performed. Contrast-enhanced abdomen CT revealed diffuse gastric wall thickening, from the esophago-gastric junction to the distal antrum (Fig. 1). A large amount of ascites with nodular thickening of the peritoneum was also observed (Fig. 1). The preliminary histopathologic results of both endoscopic biopsy and peritoneal fluid-aspiration biopsy suggested that metastatic carcinoma is possible. A 18F-fluorodeoxyglucose positron-emission tomography/computed tomography (FDG PET/CT) was performed was performed to evaluate the primary malignancy and showed increased FDG uptake in the stomach, abdominal mesentery, and the right breast (Fig. 2). A breast sonography 178revealed irregular, spiculated and hypoechoic nodules with maximum diameters measuring approximately 24 mm with a surrounding hyperechoic rim in the right upper outer breast (Fig. 3). No abnormal axillary lymph nodes were observed on sonography. Due to the patient’s poor general condition, a mammography was not possible. For the right breast nodule, sonography-guided core biopsy was performed and as a result, invasive lobular carcinoma was found (Fig. 4). The immunohistochemical staining results indicated that the estrogen receptor (ER) was positive, and the progesterone receptor (PR), CerbB2, and E-cadherin were negative. Immunohistochemical staining of endoscopic stomach biopsy specimens were positive for ER as well as PR. A histologic and immunohistochemical analysis of gastric biopsy specimens relative to breast core biopsy specimens, confirmed that gastric invasive lobular carcinoma originated from the breast (Fig. 5). The diagnosis was evident because their histologic and immunohistochemical features were so similar. The patient received chemotherapy along with adriamycin and docetaxel without surgical treatment.
DISCUSSION
Although breast cancer is the second most common type of primary tumor capable of metastasis to the stomach next to malignant melanoma, gastric metastasis from breast cancer is relatively rare (1). The clinical study series reported that the incidence of gastric metastases among breast cancer patients ranged from 0.3% to 8.0% (123). Interestingly, the predominant histologic type of breast cancer with gastrointestinal (GI) metastases is a lobular type which accounts for only 8% of all breast cancers (23). Generally, the metastatic patterns of lobular and ductal carcinoma of the breast are different, with a higher prevalence in the gastrointestinal system, gynecologic organ, and peritoneum-retroperitoneum metastases for lobular carcinoma (23). In this case study, invasive lobular carcinoma, characterized by gastric endoscopic features of diffuse infiltrative patterns with ulceration, was also observed. Gastric metastasis from breast cancer generally occurs many years after receiving breast cancer treatment. Evidently, the mean interval between the primary diagnosis of breast cancer and GI metastasis was approximately 7 years (3). The stomach may be the first site of presentation of recurrent metastatic disease of breast cancer (4567). In some cases, it may happen at the time of primary breast cancer diagnosis. Ciulla et al. (8) reported a case of stomach metastasis originating from occult breast lobular cancer, and the immunohistochemical diagnosis was primarily emphasized in order to distinguish gastric metastasis from primary gastric cancer. However, due to the mis-diagnosed endoscopic superficial biopsy, the patient underwent gastrectomy and only after an unnecessary operation was the breast cancer identified as the primary tumor (8). Consequently, the authors suggested an algorithmic use of targeted immunohistochemical markers such as the ER protein, PR protein, gross cystic disease fluid protein (GCDFP)-15, and cytokeratin (CK) 7 to determine the primary site of GI tumors. In general, an immunohistochemical analysis is regarded as the only reliable method capable of distinguishing gastric metastasis from primary gastric cancer (9). Metastatic breast cancer is positive for CK7, GCDFP-15, carcinoembryonic antigen, ER and PR, and it is negative for CK20 (89). Alternatively, ERα expression is also considered as a reliable metric for the diagnosis of gastric metastasis in breast carcinoma (89). In our case, only immunohistochemical markers of ER and PR were used and results showed ER-positive and PR-positive because specific immunohistochemical markers of CK7, GCDFP-15 and CK 20 were not available at our institution. Rather, FDG PET-CT was used as a useful alternative enabling an accurate and fast diagnosis in our case. It also showed a focal hot uptake in the right breast and diffuse, mild uptake in the stomach and abdominal mesentery. Lastly, comparison of microscopic features between endoscopic and breast core biopsy specimens enabled us to distinguish gastric metastasis from primary gastric cancer. Detection of the occult primary tumor is crucially important, since it might help in outlining a proper treatment approach, which in turn, may improve patient prognosis. Occasionally, additional diagnostic work-up, such as examining immunohistochemical markers, can be time consuming and expensive. FDG PET/CT can be an excellent and alternative whole-body imaging modality, allowing for the detection of an unknown primary tumor. However FDG PET/CT has limitations in that it can fail to detect small (< 1.0 cm) and low-grade malignant lesions (10). Moreover, breast cancer is the most common cause of false-negative results in FDG PET/CT for unknown primary tumors, and invasive lobular breast carcinomas have significantly lower FDG uptake compared with invasive ductal breast carcinomas (10). Nevertheless, FDG PET/CT was a valuable tool in the decision to manage our patient with occult primary breast invasive lobular cancer.
In conclusion, stomach metastasis could be the manifestation of occult breast cancer, even in patients without previous breast cancer history. FDG PET/CT might play an important role in the detection of occult primary breast cancer as an ancillary method to immunohistochemical studies.




 XML Download
XML Download