

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Sinonasal papillomas are benign neoplasms classified by the Hyams (1) into 3 histological types: inverted, fungiform (exophytic, septal, squamous), and cylindrical cell (oncocytic schneiderian). Inverted papilloma results from an inversion of the neoplastic epithelium into the underlying stroma (1). Fungiform papillomas are similar to papillomas commonly found in other sites along the upper respiratory tract in that they are exophytic epithelial lesions (1). The cylindrical cell papilloma, the rarest of the 3 types, accounts for only 3% to 5% of all sinonasal papillomas. It arises from the mucosa of the paranasal sinuses and nasal cavities, and is characterized by tall, columnar epithelium composed of oncocytes. The oncocytic nature of these lesions was established by Barnes and Bedetti (12) has been recognized as having a propensity for local recurrence (33-40%) and malignant transformation (4-17%) (13).
The findings of oncocytic schneiderian papilloma on conventional imaging modalities such as CT and MRI are nonspecific and may be confused with squamous cell carcinoma or even an inflammatory polyp or retention cyst. A few case reports regarding the findings of oncocytic schneiderian papilloma at 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET or PET/CT) have been documented in the English literature (4-7), but not in the Korean radiological literature.
We report here a case of oncocytic schneiderian papilloma presenting as an intensely hypermetabolic lesion on 18F-FDG PET/CT performed for cancer screening, along with sinonasal CT findings.
CASE REPORT
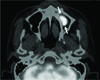
A 54-year-old man was referred to our department for further evaluation of an incidentally identified intensely hypermetabolic mass in the left maxillary sinus on 18F-FDG PET/CT. He had been regularly medicated for hypertension that 474was diagnosed 5 years prior. Approximately 3 months prior, he underwent a brain MRI for headaches, insomnia, and dizziness at another hospital, which was negative, but sinusitis was found in the left maxillary sinus. Approximately 1 month prior, he underwent 18F-FDG PET/CT using a dedicated PET/CT system (Discovery STE, GE Healthcare, Milwaukee, WI, USA) for cancer screening at our medical center, which revealed an intensely hypermetabolic [maximum standardized uptake value (SUVmax): 22.2 g/mL] mass in the left maxillary sinus (Fig. 1). Physical examinations were unremarkable except for a nasal septal deviation on the right side. Multidetector-row CT was performed using a Sensation 64 scanner (Siemens, Erlangen, Germany). The mass was isoattenuating compared with brain parenchyma or adjacent muscles on non-enhanced CT (NECT) (Fig. 2A, C). Contrast-enhanced CT (CECT) images revealed an approximately 10 × 21 × 13 mm sized, smoothly marginated mass with solid enhancement at the floor of the left maxillary sinus (Fig. 2B, D). In addition, mucosal thickening was noted in the left maxillary sinus, which is suggestive of chronic sinusitis. The solidly enhancing mass coincided exactly with intensely hypermetabolic focus on 18F-FDG PET/CT, while mucosal thickening did not show FDG uptake. Bony changes were not evident on CT (Fig. 2). On the basis of findings at 18F-FDG PET/CT and CECT, benign or malignant neoplasms were suggested as possible diagnoses. However, intense hypermetabolism on 18F-FDG PET/CT arouse malignancy suspicion. Surgical removal of the mass was performed by uncinectomy, as well as middle and inferior meatal antrostomies via the endoscopic approach. Histologic findings of the mass were consistent with oncocytic schneiderian papilloma (Fig. 3). Immunohistochemical staining showed strong expression of glucose transporter 1 (Glut-1) (Fig. 3). The postoperative course was uneventful, and there has been no evidence of tumor recurrence until 23 months after surgery.
DISCUSSION
False-positive PET scans may result from inflammatory conditions such as infection, granulomatous disease, asymmetric muscle activity, physiologic uptake, and inflammation and granulation tissue at surgical sites (89). Benign neoplasms may be another cause of false-positive PET scans. In most reported cases, the 18F-FDG PET/CT studies for sinonasal lesions were performed after biopsy. Biopsies performed close to the PET time may have led to increased FDG uptake due to inflammation from the procedure. In our case, imaging was performed before the biopsy, making it unlikely that inflammation resulting from the biopsy affected the degree of FDG uptake. Furthermore, despite its small size, the mass in our case was intensely hypermetabolic (SUVmax: 22.2 g/mL). It aroused suspicion of malignancy, which presented a clinical dilemma because the extent of surgery might be determined by the histology of the lesion.
Some investigators have reported that squamous cell carcinoma or inverted papilloma with squamous cell carcinoma showed more intense FDG uptake than benign inverted papilloma (1011); whereas, others have suggested that 18F-FDG PET/CT does not appear to reliably differentiate benign from malignant sinonasal papilloma (4). Our literature review showed that the average SUVmax of four reported oncocytic schneiderian papillomas were higher than that of inverted papillomas, inverted papillomas with squamous cell carcinoma, or squamous cell carcinomas of the sinonasal area. The reported SUVmax of the four oncocytic schneiderian papillomas in the English literature ranged from 18.9 g/mL to 43.0 g/mL (average SUVmax: 27.6 g/mL), while the reported SUVmax of inverted papilloma, inverted papilloma with squamous cell carcinoma, and squamous cell carcinoma of the sinonasal area were 2.0-9.0 g/mL (average SUVmax: 5.26 g/mL), 8.9-20.9 g/mL (average SUVmax: 14.90 g/mL), and 10.4-19.4 g/mL (average SUVmax: 13.88 g/mL), respectively. The extremely high SUVmax of oncocytic schneiderian papilloma is consistent with other oncocytic neoplasms such as oncocytomas, and oncocytic papillomas, and Hürthle cell neoplasm, all of which also show intense hypermetabolism despite their benign nature (121314), and thus reduce the specificity of 18F-FDG PET or PET/CT. The cause of increased FDG uptake in oncocytic Schneiderian papilloma is not clearly understood. It is hypothesized that oncocytic neoplasms contain abundant mitochondria ultrastructurally, which may explain the high metabolic activity and FDG uptake (15). In addition, tumor cells are associated with increased glycolysis and this metabolic property leads to increased uptake of FDG. Many studies have focused on the expression of Glut-1 and hexokinase II (HK-II) activities as correlated with FDG uptake in the various types of tumors (1617). However, there is little data on the expression of these markers and the relationship with FDG uptake in oncocytic neoplasms (18). A case of pulmonary typical carcinoid with an extensive oncocytic component showing intense uptake of FDG has been reported (18). Kadowaki et al. (18) noted that the oncocytic component was highly positively stained for Glut-1, which might be associated with the intense uptake of FDG. Our case confirmed their observations.
The CT findings of oncocytic schneiderian papilloma have not been comprehensively reviewed in the literature. Our case of onconcytic schneiderian papilloma revealed that the mass was isoattenuating compared with brain parenchyma on NECT with solid enhancement on CECT, which are nonspecific and could be seen in various benign and malignant neoplasms.
In conclusion, it is of prime importance to recognize that a sinonasal lesion with intense hypermetabolism on 18F-FDG PET/CT does not necessarily signify a malignancy. Oncocytic schneiderian papilloma should be included in the differential diagnosis of a solidly enhancing mass with intense hypermetabolism. Care must be taken to avoid the misdiagnosis of oncocytic schneiderian papilloma as a sinonasal malignancy on 18F-FDG PET/CT.


 XML Download
XML Download