

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Glomus tumors are rare benign neoplsms arising from neuromyoarterial glomus bodies (1). Most occur in a distal phalanx, often subungally, but they may be found anywhere throughout the body (12). The tumors in unusual locations-extradigial glomus tumors-are extremely rare and difficult to accurately diagnose before surgery (12345678). To our knowledge, only a few cases of extradigital glomus tumors with their radiologic findings have been reported. We report on a case of a glomus tumor unusually located in the upper arm with typical magnetic resonance imaging (MRI) and pathologic findings.
CASE REPORT
A 61-year-old man presented to our hospital with a 10-year history of pain in right upper arm, which was diagnosed as a mass. The pain became more intense with light touch or clothing, but was not related to arm movements.
On physical examination, the man made a soft, mobile, and painful lesion in the mid lateral aspect of the right upper arm, measuring 1 × 1 cm. The lesion seemed superficial, but was with no overlying skin change.
The upper extremity MRI demonstrated a well-demarcated nodule, 1.3 × 0.9 × 1.4 cm in size, located in the subcutaneous layer, mid lateral aspect of the right upper arm that showed hypointensity on axial T1-weighted images and homogeneously enhanced by injection of gadolinium. The axial T2-weighted image was hyperintense (Fig. 1).
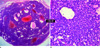
The patient underwent surgery with an initial diagnosis of a glomus tumor in an unusual location. The lesion was completely excised and a histopathologic diagnosis confirmed the clinical and radiologic diagnoses. The histologic examination showed a well circumscribed tumor located in the subcutis. is the lesion was composed of sheets of uniform cells with small amounts of eosinophilic cytoplasm, well defined cell margins, and round or ovoid puched-out central nuclei. There are dilated, cavernous-like, thin walled vascular spaces surrounded by glomus cells (Fig. 2).
The patient experienced immediate relief of pain and has remained asymptomatic without any complications or recurrence one year postoperatively.
DISCUSSION
Glomus tumors are benign hamartomatous growths of neuromyoarterial glomus bodies (1). Glomus bodies are present in the stratum reticularis of the dermis throughout the body, but they are highly concentrated in the digits, palms, and soles of the feet. Glomus tumors are composed of an afferent arteriole, arteriovenous complex, and efferent venules (2). Histologic examination reveals branching vascular channels separated by connective tissue stroma containing aggregates, nests, and masses of specialized glomus cells that have electron microscopic features of smooth-muscle cells (9).
Glomus tumors have been reported to account for 1.6% of all soft tissue tumors and 1-5% of hand tumors (10). They occur most commonly in the nail beds of the hands (1). However, a significant proportion (up to 35%) of glomus tumors are extradigital, and have been reported in many cases, including most sites of the upper and lower extremities, visceral organs, lungs, and trachea (12345678). Extradigital glomus tumors involving the upper arm have been rarely reported. In a comprehensive review of 56 patients with extradigital glomus tumors, 28 tumors (50%) were in the upper extremity, and very few cases were in the upper arm of the world's literature (2). Moreover, the discussion of the MRI findings of extradigital glomus tumors involving the upper arm is limited and restricted to case reports.
A typical glomus tumor of the hand is readily diagnosed with clinical and radiologic findings. Most of the tumors in the subungal locations present the classic symptom triad of pain, pinpoint tenderness, and hypersensitivity to a cold (1). Ultrasonography and MRI have been used to localize and characterize the tumors. As a first line method, ultrasonography is helpful to detect the lesion, despite its low specificity and tumor presentation as a well-defined hypoechoic mass (568). MRI has proven to be the most sensitive imaging modality for the diagnosis of glomus tumors and was most successful when a radiographic marker was placed directly over the exact point where the patient experienced pain (2). MRI also gives more details of the lesion and its relationship to adjacent structures, which facilitated complete removal by excision (8). The typical appearance of glomus tumors on MRI is a circumscribed mass of intermediate or low signal on T1-weighted images and high signal on T2-weighted images, with diffuse enhancement after gadolinium administration (2).
The diagnosis of extradigital glomus tumors remains a challenge. Their unusual location and nonspecific clinical findings, except for pain, make the diagnosis difficult. Therefore, history, clinical examination and proper radiologic examination are essential (4).
In this case, the patient presented specific pain and the lesion was palpable superficially on physical examination. Therefore, clinicians could suspect glomus tumors. For further evaluation and differential diagnosis of the lesion, MRI was performed with the radiologic marker on the painful site. The lesion showed typical MRI findings of the glomus tumor with characteristic signal changes and enhancement pattern.
The broad differential diagnosis includes a neural tumor such as a neurofibroma, vascular tumor including hemangioma, angioma, or hemangiopericytoma, as well as a leiomyoma or metastasis (6). A glomus tumor should be considered in the differential diagnosis of any painful soft tissue mass (8).
In conclusion, we presented a histologically proven extradigital glomus tumor in the upper arm. Presurgical MRI depicted lesion characteristics and location. Radiologists should be aware of the existence of these lesions, particularly in the setting of chronic pain and focal tenderness. This rare differential should be considered, despite its unusual location.

 XML Download
XML Download