

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bizarre parosteal osteochondromatous proliferation (BPOP) is a rare benign lesion arising from the surface of cortical bone which usually occurs in the small bones of distal extremities and shows exophytic growth. Such a lesion can be cured by local excision. BPOP can be confused with some benign and malignant diseases such as osteochondroma, paraosteal osteosarcoma, or chondrosarcoma, both radiologically and pathologically (1). We illustrate imaging features including simple radiograph and magnetic resonance imaging of BPOP in the proximal phalanx of the hand with unusual cortical erosion and bone marrow edema accompanied by soft tissue enhancement.
CASE REPORT
A 10-year-old female presented with a palpable mass in the volar aspect of her right 2nd finger at the level of the proximal interphalangeal joint. The mass had appeared over 6 months without pain. She did not have underlying joint disease or history of trauma. Physical examination revealed a round, firm, non-tender, fixed mass with intact overlying skin in her 2nd finger.
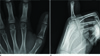
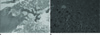
Plain radiographs showed a well-defined exophytic osseous mass arising from volar aspect of the right 2nd proximal phalangeal shaft (Fig. 1). The mass had a sessile appearance with peripheral sclerosis in the underlying bony cortex and no mineralization in the lesion or continuity with the medulla was evident. Subsequent MRI showed a well-defined ovoid paraosteal mass with erosion in the cortex and medulla of the 2nd proximal phalangeal shaft measuring 3.4 × 3.7 cm. The mass had iso-signal intensity to muscle on T1-weighted images and high signal intensity on T2-weighted images with T1, T2 low signal intensity rim, corresponding to sclerotic rim on simple radiograph (Fig. 2). Surrounding soft tissue and bone marrow edema were seen on T2 weighted images. The lesion and adjacent soft tissue showed well enhanced on gadolinium-enhanced T1 fat suppression sequences.
An excisional biopsy was performed which, upon microscopic examination, revealed a mixture of hypercellular cartilage maturing to trabecular bone with a classic irregular chondro-osseous interface seen in the resected mass (Fig. 3). There was irregular maturation of cartilage with hypercellular, occasional binucleated, enlarged chondrocytes. The irregular woven bone was surrounded by fasciitis-like spindle cell proliferation without atypia. Woven and lamellar bones were covered by rims of osteoblast. There was no evidence of local recurrence, both clinically and radiologically in the follow-up period of 11 months.
DISCUSSION
BPOP, also known as Nora's lesion, is a rare benign lesion occurring in small bones of the hand and foot with no sex predilection. BPOP can occur at any age, but most often occurs in 20-30 years old patients (123). Overall, about three quarters of cases of BPOP affect small bones of distal extremities including proximal shafts of the phalanges, metacarpals and metatarsals, and rarely, distal phalanges. Also, BPOP affects large bones less commonly (-27% of cases) (4), and usually presented with a painless and slowly enlarging lump. BPOP is known as a reactive lesion of the bone surface with florid reactive periostitis, or turret exostosis, depending on temporal factors, local anatomical features, and breaching of the periosteum.
On plain radiograph, BPOP appears as a well-defined calcified osseous mass attached to the cortex by a broad base without cortical erosion. Usually, cortical erosion, continuity with medullary cavity, and disturbance of underlying bone are not seen in BPOP lesions. Radiologic findings of osteochondroma and BPOP may be difficult to distinguish. However, osteochondroma is uncommon in distal extremities and appears to have a typical orientation away from the physis, and has continuity within the medullary cavity. BPOP resembles osteochondroma in gross specimen, but the latter is typically covered by a cartilaginous cap with enchondral ossification (2). Lack of medullary continuity in BPOP on CT scans helps to distinguish between these two diseases with certainty.
MRI is useful in characterizing the plain features of BPOP, revealing low signal intensity on T1 sequences with uniform enhancement following gadolinium administration, and a variable signal on fast spin echo T2-weighted images, gradient sequences, and STIR sequences according to the relative amount of cartilage in the lesion. Usually, BPOP has no adjacent soft tissue swelling, cortical destruction, medullary involvement or stress fracture (1). These findings help to further differentiate BPOP from malignant tumors or other reactive lesions of bone surface.
The case presented here shows unusual aggressive findings of BPOP on MRI, which included cortical erosion of underlying bone with bone marrow edema and enhancement in the adjacent soft tissue. These features can lead us to preoperative misdiagnosis of the lesion to periosteal chondroma with inflammation, florid reactive periostitis, or rarely, of eosinophilic granuloma due to the patient's young age. Several cases of BPOP with atypical radiologic features such as cortical destruction, irregularity, medullary continuity, and periosteal reaction have been reported (5). Because a feature like cortical erosion is usually seen in primary bone tumor, it is suggested that BPOP is a benign neoplastic lesion rather than a reparative/reactive process after periosteal injury.
Several hypotheses about the etiology of BPOP have been suggested; Ly et al. (6) reported a case of BPOP developing after injury. However, in other studies, it was reported that traumatic events preceded in about 30% of the cases of BPOP (7). Therefore, preceding trauma history is not always consistent in BPOP patients. Yuen et al. (8) suggested the "unitary hypothesis", which is BPOP, may be a part of a spectrum of reactive lesions with different degrees of maturation. Translocation between chromosomes 1 and 17 has been reported to be a distinct translocation point unique to BPOP. However, Sakamoto et al. (9) reported the inversion of the long arm of chromosome 7 in BPOP and variant chromosomal abnormalities in BPOP, which may be related to the different phenotypes such as corticomedullary continuity. Joseph et al. (3) also reported abnormal karyotypes including abnormalities at chromosome 6, 7 and t (1 : 17), which may not be the only distinct translocation point. These genetic abnormalities support that BPOP is a neoplastic lesion and exclude the unitary hypothesis. Histologically, BPOP is composed of bone, fibrous tissue and cartilage (10). Irregular maturation of cartilage in bone produces chondro-osteoids with a characteristic blue quality. BPOP contains enlarged, bizarre, binucleated chondrocytes with maturation into bone. In addition, there is proliferation of spindle cells between bony trabeculae without atypia. In contrast, there are more regular alignments of chondrocytes in osteochondroma and hyperchromasia and cytological atypia in malignant lesions such as osteosarcoma or chondrosarcoma.
Asymptomatic lesions may be followed up with radiologic study. However, a surgical resection is needed in symptomatic cases (6). Excision with a wide resection margin in a case of BPOP with cortical erosion has been reported. The recurrence rate of BPOP ranges up to 55%, therefore, long term follow-up after the excision with simple radiograph is necessary (11). And, if there are findings suggesting an increase in the size of the lesion, adjacent soft tissue swelling, or cortical irregularity, further evaluation with CT or MRI is necessary.
This case of BPOP in the proximal phalanx showed unusual radiologic findings of cortical erosion and medullary involvement with adjacent soft tissue edema and enhancement on MRI. In conclusion, it is important to be aware of these unusual findings of BPOP mimicking malignancy to avoid aggressive treatment.

 XML Download
XML Download