

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To evaluate the relationship between the degree of scoliotic curvature and postoperative change of the chest wall among patients who underwent a unilateral mastectomy.
Materials and Methods
Subjects were comprised of 56 women who underwent chest CT and a whole spine standing anteroposterior view (WSSAP). Cobb's angle and each side of the chest wall volume, including the breast, were measured with the WSSAP and a 3-D reconstructed multi-detector computed tomography (MDCT) image. A correlation analysis was performed between the scoliotic curvature and chest wall volume asymmetry. Directional correspondence between development of scoliosis and undergoing a mastectomy was analyzed. Furthermore, a survey on patient shoulder function was performed using a questionnaire and a correlation was performed between the results of the survey and the scoliotic curvature and chest wall volume asymmetry.
Results
The findings indicate that Cobb's angles were 4.4° ± 2.7 (Mean ± SD, range from 0.6 to 11.4). Differences in chest wall volume were 474.64 ± 276.36 cm3 (Mean ± SD, range from 78 to 1379). No statistical significance was noted between the degree of scoliotic curvature and chest wall volume asymmetry (p > 0.05). A cross-tabulation analysis of the direction between the scoliotic curvature and mastectomy was found to be statistically significant (p < 0.001). Also, there was a significant correlation between shoulder function assessment score and the degree of scoliotic curvature (p = 0.003), while no significant correlation between shoulder function assessment score and chest wall volume asymmetry (p = 0.091) could be found.
Figures and Tables
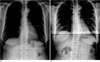 | Fig. 1Measuring Cobb's angle by Cobb method of 44 years old female patient.
A. Preoperative chest plane radiograph.
B. Whole spine standing anteroposterior view after 4 years.
|
 | Fig. 2Measured volume of the chest wall by 3D reconstructed volume rendering image of chest MDCT.
A. Whole chest wall volume is divided into 4 segments by right anterior (RtA), left anterior (LtA), right posterior (RtP), left posterior (LtP).
B. The muscle volume of chest wall is measured with 20-80 HU threshold (mRtA, mLtA, mRtP, mLtP).
Note.-MDCT = multi-detector computed tomography
|

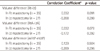
Table 2
Chest Wall Volume Differences in Mastectomy Patients by Chest MDCT with 3D Volume Reconstruction

![]()

References
1. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer Statistics, 2008. CA Cancer J Clin. 2008; 58:71–96.
2. Ministry for Health, Welfare and Family Affairs. Annual Report of cancer incidence (2007), cancer prevalence (2007) and survival (1993-2007) in Korea. Seoul: Ministry for Health, Welfare and Family Affairs;2009.
3. Won YJ, Sung J, Jung KW, Kong HJ, Park S, Shin HR, et al. Nationwide cancer incidence in Korea, 2003-2005. Cancer Res Treat. 2009; 41:122–131.
4. Kuehn T, Klauss W, Darsow M, Regele S, Flock F, Maiterth C, et al. Long-term morbidity following axillary dissection in breast cancer patient--clinical assessment, significance for life quality and the impact of demographic, oncologic and therapeutic factors. Breast Cancer Res Treat. 2000; 64:275–286.
5. Bower JE, Ganz PA, Desmond KA, Bernaards C, Rowland JH, Meyerowitz BE, et al. Fatigue in long-term breast carcinoma survivors: a longitudinal investigation. Cancer. 2006; 106:751–758.
6. Bendz I, Fagevik Olsén M. Evaluation of immediate versus delayed shoulder exercise after breast cancer surgery including lymph node dissection--a randomised controlled trial. Breast. 2002; 11:241–248.
7. Wingate L. Efficacy of physical therapy for patients who have undergone mastectomies. A prospective study. Phys Ther. 1985; 65:896–900.
8. Aebi M. The adult scoliosis. Eur Spine J. 2005; 14:925–948.
9. Lee SW, Lee TJ, Lee SW. Does unilateral mastectomy cause scoliosis? J Korean Soc Plast Reconstr Surg. 2008; 35:279–282.
10. Shamley D, Srinaganathan R, Oskrochi R, Lascurain-Aguirrebeña I, Sugden E. Three-dimensional scapulothoracic motion following treatment for breast cancer. Breast Cancer Res Treat. 2009; 118:315–322.
11. Cheville AL, Tchou J. Barriers to rehabilitation following surgery for primary breast cancer. J Surg Oncol. 2007; 95:409–418.
12. Hagay C, Cherel PJ, de Maulmont CE, Plantet MM, Gilles R, Floiras JL, et al. Contrast-enhanced CT: value for diagnosing local breast cancer recurrence after conservative treatment. Radiology. 1996; 200:631–638.
13. Lindfors KK, Meyer JE, Busse PM, Kopans DB, Munzenrider JE, Sawicka JM. CT evaluation of local and regional breast cancer recurrence. AJR Am J Roentgenol. 1985; 145:833–837.
 XML Download
XML Download