

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Myoepitheliomas are rare benign tumors composed entirely of myoepithelial cells with no ductal differentiation (1) and account for 1.5% of all tumors in the major and minor salivary glands of which, 40% of these arise in the parotid glands (12). Only a few reports of myoepitheliomas occurring only in the soft palate exist in the literature. Here, we report the appearance of a myoepithelioma in the soft palate on CT and MRI.
CASE REPORT
A 53-year-old woman visited the department of otorhinolaryngology in our hospital with a palpable mass on the soft palate that had existed for several years. A round, movable, pinkish mass originating from the right posterior portion of the soft palate was found during physical examination. The attending physician ordered an imaging evaluation to determine the tumor diagnosis and location. On the non-contrast enhanced CT scan, the mass had a smooth and partial lobulating contour, and was approximately 3.5 cm in size. The tumor was located in the right soft palate and had slightly compressed the right parapharyngeal space.
Contrast-enhanced CT was performed; after administering 90 mL of contrast material into an antecubital vein at a rate of 3 mL/sec with a power injector, enhanced images were obtained with a scanning delay of 35 sec. The contrast enhanced CT images showed faint contrast enhancement inside the mass while the periphery of the mass was moderately enhanced (Fig. 1). We assumed that moderate peripheral enhancement was due to the capsular structure of the mass. Magnetic resonance imaging was performed for further evaluation. On the T1-weighted images, the mass had slightly heterogeneous, iso-signal intensity compared to the pharyngeal muscle. The mass was clearly visible on the T2-weighted images, and was heterogeneous with high signal intensity along with a smooth and partial lobulating contour. The tumor was heterogeneously enhanced on the Gd-enhanced T1-weighted images and had a partial non-enhancing portion (Fig. 2).
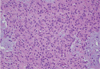
The patient underwent tumor resection under general anesthesia and the specimen was a grayish brown soft tissue mass measuring 3.5 × 2.5 × 2.0 cm. Once sectioned, the tumor was found to be mainly solid with some necrotic changes. We believe that the non-enhancing portion of the tumor on the Gd-enhanced T1-weighted images was consistent with the intratumoral necrotic portion. Haematoxylin and Eosinstained sections of the resected mass showed marked plasmacytoid cell proliferation, polygonal cells with eccentric nuclei, and abundant hyaline eosinophilic cytoplasm in the myxoid tustroma background (Fig. 3). S-100 protein and cytokeratin immunostaining was strongly positive in the tumor cells, whereas smooth muscle actin staining was focally positive in the tumor cells. These histologic and immunostaining observations were consistent with plasmacytoid myoepithelioma.
DISCUSSION
Myoepithelioma is a benign tumor composed of sheets and islands of various proportions of spindle, plasmacytoid, epithelioid, and clear cells that exhibit myoepithelial but not ductal differentiation (3). Myoepithelioma was initially considered to be a subtype of pleomorphic adenoma, but was later distinguished from other types of pleomorphic adenoma. This type of tumor has been classified as a distinct clinicopathological entity by the World Health Organization since 1991 (4). Myoepithelioma may originate from the salivary gland, lacrimal gland, breast, bronchus, or skin. The most common location of myoepitheliomas is the salivary gland, particularly the parotid gland. Myoepitheliomas account for less than 1% of salivary gland neoplasms (4). The ages of patients with myoepitheliomas range from 9 to 85 years, with an average of 44 years; this disease occurs most commonly among patients in their 30s (2).
A few reports have described the appearance of myoepithelioma in the soft palate on CT and MRI. Monzen et al. (5) reported CT and magnetic resonance imaging features of myoepithelioma arising from the soft palate. In this report, benign myoepiethelioma was found to have a smooth surface and faint contrast enhancement inside the mass on contrast-enhanced CT images. This lesion appears as a well-defined ovoid mass with iso-signal intensity compared to muscle on T1-weighted images. On T2-weighted images, the mass appears as an area with high signal intensity while the well-enhanced periphery of the mass shows low T2-signal intensity, suggesting a capsular structure. Slightly heterogeneous enhancement of the mass is evident on contrast-enhanced T1-weighted images. Such findings are similar to our case and we can assume that the imaging features of our patient were consistent with myoepithelioma.
There are many biologic factors that influence the enhancement patterns of tumors such as vascularity and histological components. We believe that faint enhancement inside the mass on contrast-enhanced CT images corresponded to the plasmacytoid cells and surrounding myxoid stroma occupying the greater part of the tumor (1). Furthermore, intratumoral necrosis showed poor enhancement on the contrast-enhanced CT and Gd-enhanced T1-weighted images. The intratumoral necrotic portion was suspected of representing malignant changes of myoepithelioma. There are several pathologic findings associated with malignancy including infiltrative growth, necrosis, cytologic atypia, high mitotic rates, and cellular pleomorphism (78). Thus, the lesion in our patient had uncertain malignancy potential; because, although there was focal necrosis, there were no other pathologic findings that suggested malignancy.
Palatal masses may be associated with many diseases including minor salivary gland tumors, neurinoma, haemangioma, malignant tumors originating from the oral mucosa, and inflammatory disease (6). However, it is easy to distinguish inflammatory from neoplastic diseases based on clinical findings such as fever or tenderness. Minor salivary glands are located everywhere in the oral mucosa. Thus, minor salivary gland tumors are primarily located in the palate (50%), lips (15%), cheek mucosa (12%), tongue (5%), and floor of the mouth (5%). Minor salivary gland tumors are a heterogeneous group of neoplasms with a broad range of histological types, occurring in the minor salivary gland. The soft palate is the second most common site of minor salivary gland tumors. The most common histological type of minor salivary gland tumors is pleomorphic adenoma. Myoepithelioma is also a rare histologic type of minor salivary gland tumor (9).
It is difficult to differentiate myoepithelioma from other tumors based on radiological findings. Histopathologic studies area needed to differentially diagnose myoepitheliomas. Some imaging studies have suggested that myoepitheliomas contain a relatively large cystic component compared to pleomorphic adenomas. Additionally, pleomorphic adenomas show relatively delayed enhancement patterns on contrast-enhanced CT images (12). We suggest that when there is a submucosal soft palate mass, radiologists should consider myoepitheliomas in the radiological differential diagnosis of soft palate tumors.


 XML Download
XML Download