

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Most described male breast lesions, such as gynecomastia, are benign. The overall incidence of male breast cancer is less than 3%. Like women, common presentations of male breast diseases are palpable lumps or tenderness. Physical examination, mammography and ultrasound are generally used for work-up of breast diseases in both women and men. However, men do not undergo screening mammograms; all male patients are examined in symptomatic cases only. Therefore, all male breast examinations are diagnostic, whereas the majority of the examinations for women are for screening purpose. The differentiation between benign and malignant breast lesions is important, especially for men, because the reported prognosis of male breast cancer is poor due to delayed diagnosis. In this article, we review the spectrum of male breast diseases, from benign to malignant, and illustrate their ultrasonographic and mammographic imaging features.
Figures and Tables
 | Fig. 1Normal male and female breast. The normal male breast is characterized primarily by subcutaneous fat without glandular tissue.
|
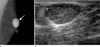
 | Fig. 2Invasive ductal carcinoma in a 53-year-old man.Mammography (A) shows an irregular, hyperdense mass with mild skin thickening.
Ultrasound (B) demonstrates a lobular heterogeneously hypoechoic mass with an echogenic dot (arrow) within the mass, representing calcification and overlying skin is thickened.
Color Doppler image (C) shows focal increased vascularity in periphery of the mass.
A suspicious metastatic lymph node (D) is also seen in the axilla.
|
 | Fig. 3Nodular gynecomastia (type 1) in a 48-year-old man.Mammogram (A) shows a small fan-shaped density radiating from the nipple.
On ultrasound (B), small amount of glandular tissue is seen.
|
 | Fig. 4Dendritic gynecomastia (type 2) in a 18-year-old man.Mammogram (A) shows retroareolar soft-tissue density with prominent extensions that radiate into the deeper adipose tissue and ultrasound (B) reveals a hypoechoic lesion with finger like posterior margin.
|
 | Fig. 5Diffuse gynecomastia (type 3) in 16-year-old man.The breast appears similar to female breast which shows heterogeneously dense parenchymal pattern on mammography (A).
Ultrasound (US) (B) also show normal glandular tissue lying between the pre- and retro-mammary fascial plane like a normal female breast US.
|
 | Fig. 6Fibrocystic change in 74-year-old man. Left MLO view shows isodense nodular asymmetry in subareolar area. This lesion was surgically confirmed to be fibrocystic changes.Note.-MLO = mediolateral oblique
|
 | Fig. 7Bilateral fibrocystic change in a 17-year-old man.Ultrasound (A, B) shows well circumscribed slightly hypoechoic lesions in the both breasts.
The microscopic finding (C) shows cystic dilatation of ducts and fibrosis (× 100).
|
 | Fig. 8Fibroadenoma in 59-year-old man.Transverse ultrasound image (A) of the right subareolar region shows relatively round, hypoechoic mass (arrow). The mass is composed of benign looking ducts and periductal myxoid stroma (B, × 200).
|
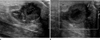
 | Fig. 9Granulomatous mastitis in a 55-year-old man with a palpable mass.A lobulated marked hypoechoic dumbbell shaped mass is seen on ultrasound (A, B).
It shows noncaseating granuloma composed of epitheloid histiocytes and lymphoplasma cells (C, × 100).
|
 | Fig. 10Cavernous hemangioma in a 66-year-old man.Left MLO view (A) shows a well-defined, hyperdense mass in the superior aspect of nipple.
Calcifications (arrow) are visible within the mass. Ultrasound (B) reveals an ovoid, well-circumscribed, hypoechoic mass with echogenic dots and innumerable anechoic lesions.
Note.-MLO = mediolateral oblique
|
 | Fig. 11Subareolar abscess in a 58-year-old man.An irregular mixed echoic mass with marked skin thickening is visible in left breast on ultrasound (US) (A).
Color Doppler US (B) image shows some increased vascularity at peripheral solid portion of the mass. It was surgically confirmed to be an organizing abscess and fat necrosis.
|


References
1. Appelbaum AH, Evans GF, Levy KR, Amirkhan RH, Schumpert TD. Mammographic appearances of male breast disease. Radiographics. 1999; 19:559–568.
2. Chen L, Chantra PK, Larsen LH, Barton P, Rohitopakarn M, Zhu EQ, et al. Imaging characteristics of malignant lesions of the male breast. Radiographics. 2006; 26:993–1006.
3. Günhan-Bilgen I, Bozkaya H, Ustün EE, Memiş A. Male breast disease: clinical, mammographic, and ultrasonographic features. Eur J Radiol. 2002; 43:246–255.
4. Wise GJ, Roorda AK, Kalter R. Male breast disease. J Am Coll Surg. 2005; 200:255–269.
5. Shetty MK, Shah YP. Sonographic findings in focal fibrocystic changes of the breast. Ultrasound Q. 2002; 18:35–40.
6. Gateley CA. Male breast disease. The Breast. 1998; 7:121–127.
7. Kook SH, Kim MS, Pae WK. Atypical sonographic patterns of fibroadenoma of the breast: pathologic correlation. J Korean Radiol Soc. 1999; 40:597–602.
8. Reddy KM, Meyer CE, Nakdjevani A, Shrotria S. Idiopathic granulomatous mastitis in the male breast. Breast J. 2005; 11:73.
9. Hovanessian Larsen LJ, Peyvandi B, Klipfel N, Grant E, Iyengar G. Granulomatous lobular mastitis: imaging, diagnosis, and treatment. AJR Am J Roentgenol. 2009; 193:574–581.
10. Vourtsi A, Zervoudis S, Pafiti A, Athanasiadis S. Male breast hemangioma--a rare entity: a case report and review of the literature. Breast J. 2006; 12:260–262.
 XML Download
XML Download