

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Angioleiomyomas are a benign soft tissue tumor arising from smooth muscle cells of blood vessels. It is also known as an angiomyoma, vascular leiomyoma or dermal angioma. This tumor is relatively rare and typically presents as a small (maximum diameter < 2 cm), freely movable, painful mass (12). Although angioleiomyomas are most frequently reported in the lower extremity and in middle-aged female patients, they can be found throughout the body in male and female adults of all ages. We report a case of an angioleiomyoma of the left 3rd digit in a 31-year-old man.
Case Report
A 31-year-old man presented with a progressive enlarged palpable mass at the left 3rd finger. He reported that the mass was palpable for about 2 years, and progressively increased in size. The man did not complain of any pain in the area. Upon physical examination, we discovered a soft, movable non-tender mass measuring approximately 3 × 2 cm and with a volar aspect of the proximal phalanx of left 3rd finger. Range of motion of the left 3rd finger was intact, though plain radiography demonstrated soft tissue swelling at the volar aspect of the left 3rd proximal phalanx without any bony abnormalities. Sonography revealed a solid, oval and well defined mass about 2.5 cm in diameter. The mass was located just above the flexor tendon, but did not appear to be attached to the tendon. The mass showed a relatively heterogeneous, hypoechoic echo texture with posterior acoustic enhancement (Figs. 1A, B). Color Doppler evaluation revealed multiple vascular channels within the mass (Fig. 1C). On MRI, the mass showed homogeneous iso-signal intensity on T1 weighted image and heterogeneous high signal intensity with a thin low signal capsule on a T2 weighted image, and multiple serpentine or linear low signal structures (Figs. 2A, B). The mass showed strong enhancement, especially peripherally on the gadolinium enhanced T1 weighted image (Fig. 2C).
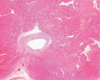
A tumor resection was performed, and a well circumscribed mass was identified in the subcutaneous tissue and over the flexor tendon of the 3rd digit. No invasion of the adjacent tendon was present and upon microscopic examination, the mass was demarcated by a fibrous thin capsule, and showed multiple tortuous small sized vessels surrounded by compact smooth muscle cells with dense fibrosclerotic tissue (Fig. 3). The pathologic diagnosis was a solid type angioleiomyoma.
Discussion
Angioleiomyomas are a rare form of leiomyoma. Leiomyomas are a benign smooth muscle neoplasm that frequently occurs in extraskeletal sites such as the ovaries, uterus, bladder, lung, and gastrointestinal tract. Occasionally, the skin and subcutaneous soft tissues are involved, as in cases of angioleiomyoma arising from the smooth muscle of small blood vessels.
Angioleiomyomas are sharply demarcated spherical masses, mostly measuring less than 2 cm in diameter (12). The peak incidence is in the fourth to sixth decades of life (1). The lower extremity tumors occur in women twice as frequently as in men, and the upper extremity tumors occur more frequently in men than in women (1). Pain is experienced more often in tumors located in the lower extremity than in an upper extremity, the head or neck (12).
Angioleiomyomas are classified into three histological types: solid, venous and cavernous (3). Solid angioleiomyomas, described as closely compact smooth muscle and many small split-like vascular channels, occur three times more in females than males and are generally the most common type. Venous angioleiomyomas, described as having thick and easily identifiable muscular walls, occur more commonly in males. Cavernous angioleiomyomas, described as having dilated vascular channels with less smooth muscle cells, are the least common type. Although angioleiomyomas are classified into three main types on pathologic examination, the MRI features are similar to differentiate among the three types of angioleiomyomas (4).
Several studies have reported about the correlation between pathology and MR findings. Hwang et al. (4) suggested that the smooth muscle and numerous vessels corresponded to the hyperintense areas, and the fibrous tissue appeared isointense on T2 weighted MR images. In addition, a well defined peripheral, hypointense rim on T2 weighted images showed fibrous capsule and the interlacing isointense areas within the tumor, which were correlated with the various amounts of connective tissue and intravascular thrombus. Yoo et al. (5) suggested that the presence of tortuous vascular channels surrounded by smooth muscle bundles and areas of myxoid change explains the heterogenicity of signal intensity in the tumor on T2 weighted images. Some tumors showed predominant myxoid change and hyalization corresponding more so to the higher signal intensity on T2 weighted image than the remaining part of mass. On gadolinium-enhanced T1 weighted images, most of the tumors showed homogeneous high enhancement; however, some only showed peripheral enhancement, which reflected the fewer vessels in the tumor tissue (5). One case report of MRI findings described tortuous vascular channels surrounded by smooth muscle bundles that corresponded to tortuous low signal intensity on T1 and T2 weighted images, which was consistent with the diagnosis of angioleiomyoma (6).
In our case, the mass showed multiple vascular structures on Doppler sonography, and serpentine or curvilinear low signal intensity structures that were thought to be tortuous vascular channels seen on T1 and T2 weighted images. Upon microscopic examination, the low signal intensity rim on T2 weighted image was found to be well correlated with fibrous capsule and the heterogenicity on a T2 weighted image corresponded to multiple vascular channels and dense fibrosclerotic tissues
The differential diagnosis may include giant cell tumors of the tendon sheath, neurogenic tumor, and hemangioma. Compared to an angioleiomyoma, a giant cell tumor of the tendon sheath frequently shows low signal intensity on T2 weighted images and an intimate relationship with the tendon sheath. Neurogenic tumors usually present as well demarcated masses of high signal intensity on T2 weighted images, but do not show tortuous vascular structure. Hemangiomas can also at times show tortuous vascular channels and well defined nodular appearance, but usually show a lobulated contour, infiltrative margin, and relatively high signal intensity on T1 weighted images due to the fatty component within the mass (7). Internal calcification and saccular vascular structure with or without thrombosis are also helpful for differential diagnosis (7).
In conclusion, we suggest that the angioleiomyoma be considered when multiple vascular structures are noted in a well defined soft tissue mass arising from the subcutaneous tissue of the extremities on MRI and Doppler sonography.


 XML Download
XML Download