

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Intraspinal cystic lesions can be widely recognized due to the remarkable advances in modern MR imaging techniques. Varying terms are ascribed to intraspinal cysts located near the facet joints including synovial cysts (1), ganglion cysts (2), and pseudocystic lesions (3). Kusakabe et al. (4) reported that a cyst, which does not have synovial lining cells but does have a communicating channel between the cyst and the neighboring facet cyst, should be simply called a 'facet cyst' (4). The exact cause for the development of a facet cyst is still not clear, but many researchers have suggested that facet cyst formation might be related to several factors including facet joint instability, trauma, and facet joint degeneration (4). Up to now, 32 cases of juxtafacet cyst hematoma in the lumbar spine have been reported in the literature. Most of them were located in the posterolateral spinal canal at the L3/4 level or lower (56). In a strict sense, only 4 cases of facet cyst hematomas have been reported in the lumbar spine (7), but to date, none have been reported in the thoracolumbar area. A facet cyst hematoma can also compress nerve roots or dura mater and cause radiculopathy or cauda equina syndrome. MRI findings of facet cyst hematomas vary depending on the biochemical form of hemoglobin, deoxyhemoglobin, methemoglobin, and hemosiderin (4). We report radiological findings of a facet cyst hematoma in the T12-L1 level and discuss the clinical course, treatment, and its possible pathogenesis.
Case Report
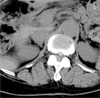
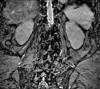
A 69-year-old female presented with complaints of back pain and Rt. lower extremity pain, as well as numbness and weakness for 3 years. The patient had no history of trauma and her medical history was otherwise unremarkable. On neurological examination, her muscle strength, deep tendon reflexes of the lower extremities, as well as bladder and bowel function were all intact. A CT scan showed an extradural mass lesion of the Rt. posterolateral region at the T12-L1 disc level and revealed a significant degenerative change of the neighboring facet joint (Fig. 1). The extradural mass exhibited heterogeneous signal intensity on both T1- and T2-weighted images in the Rt. posterolateral spinal canal and was attached to the Rt. T12-L1 facet joint (Fig. 2). This mass lesion compressed the posterolateral surface of the spinal cord at the same level. A MR myelography showed a heterogeneous mass lesion continuing to the neighboring facet joint at the same level (Fig. 3). With the patient under general anesthesia, a T12/L1 laminectomy and right T12/L1 medial facetectomy were performed. Intraoperatively, the extradural mass, which was covered with a very thin membrane, was directly visualized and was continuous to the neighboring facet joint. It was filled with dark hemorrhage. A histological examination revealed that the wall of the mass was composed of very thin fibrous connective tissue without synovial lining cells (Fig. 4). There was no evidence of a ganglion cyst or ligament flavum cyst. The content was pure hemorrhage. After surgery, the patient's symptoms resolved and her neurological function was normalized.
Discussion
With the remarkable advances in imaging techniques, the incidence of intraspinal cystic lesions has increased. Chisako et al. (8) classified intraspinal epidural cysts into two categories depending on whether they were located near a facet joint capsule: 1) juxtafacet cysts (synovial cysts, ganglion cysts, and ligament flavum cysts, which are almost always attached to the periarticular connective tissue of facet joint); 2) other cysts (cystic lesions that are not always located near a facet joint, such as neurogenic cysts, arachnoid cysts, and meningeal cysts) (8). Since Hsu et al. (9) first used the term "intraspinal facet cyst" (9), several authors had tried to define a facet cyst. Chisako et al. (8) insisted that three types of juxtafacet cysts should come under the category of facet cyst because of the impossibility of clearly distinguishing between juxtafacet cysts due to synovial lining cell degeneration and disappearance, and the change in synovial fluid consistency owing to hemorrhage and inflammation (8) However, Kusakabe et al. (4) defined facet cysts more strictly as a cyst located beside the facet joint without synovial lining cells or gelatinous fluid, and in communication with the neighboring facet joint, as confirmed by arthrography and a CT scan (4). A number of juxtafacet cysts have been reported, but only 32 cases among them showed a hemorrhage into the cysts (256,10). Most cases suffering from a juxtafacet hematoma complained of severe pain due to the acute enlargement of the cyst by hemorrhage and subsequent nerve root compression. Strictly speaking, only 4 cases of facet cyst hematoma in the lumbar spine have been reported in the literature (7). They were located in the posterior or posterolateral part of the spinal canal at the L3/4 or lower level and commonly presented with chronic radicular symptoms. In our case, the facet cyst hematoma occurred in the thoracolumbar area and the clinical course was not abrupt. The pathogenesis of facet cyst formation is not clear. Several authors reported that facet cyst formation was related to the instability of the facet joint (249). The pathophysiology of these lesions may involve facet degeneration and focal weakness areas in the joint capsule caused by repetitive motion due to instability. This is followed by herniation of the synovium and the formation of a synovial cyst. This hypothesis is supported by evidence that many facet cysts remain in continuity with the facet joint, as evidenced by arthrography or by the presence of air within both the cyst and joint. Further support is found in the observation that the majority of facet cysts occur at L4-5, the level with the greatest facet mobility (1). Our case was found at the T12-L1 interspaces, which might be considered the transitional zone between the relatively immobile thoracic segments and highly mobile lumbar segments. Such differences in the degree of mobility between the neighboring spinal segments at the thoracolumbar junction may increase the biomechanical loading and tortional stress, hence accelerating the degenerative changes in the thoracolumbar junction facets. Other possible causes are trauma or chronic microtrauma. In our case, a preoperative CT scan showed severe facet joint degeneration at the T12/L1 level, but there was no evidence of trauma.
The cause of a facet cyst hematoma is still unclear. It may arise from vessel breakage around the pre-existing facet cyst caused by facet instability. Synovium is a vascular rich tissue and the number and volume of vessels may increase in a degenerative joint cavity. The secretion of angiogenic factors by synovial cells likely mediates this increase (5). Accordingly, it can be theorized that minor trauma which patients are unconscious of, could cause bleeding from these capillary vessels. In response to greater exercise loading and more advanced tissue degeneration, hemorrhagic episodes may occur in a repeated manner.
MR imaging is effective in the diagnosis of a facet cyst hematoma. The signal intensity of a facet cyst hematoma varies over time: 1) during the acute stage, the hematoma is isointense relative to the spinal cord on T1-weighted images and hyperintense relative to the spinal cord on T2-weighted images. 2) during the subacute stage, such as 30 hours after symptom onset, the hematoma usually has a heterogeneous hyperintensity on both T1- and T2-weighted images. The increased heterogeneity of the hematomas results from the degradation products of hemoglobin. Our case showed heterogeneous hyperintensity on both T1- and T2-weighted images, suggesting that the hematoma is in the subacute phase with methemoglobin. The hematoma continued to the neighboring facet joint and the same signal intensity was observed at the neighboring facet joint space (Fig. 4). Kusakabe et al. (4) insisted that a facet cyst should be confirmed by arthrography and a CT scan, but a preoperative MR myelography may also be helpful in diagnosing a facet cyst when there is direct communication between the cyst and facet joint. Microscopically, synovial lining cells or gelatinous fluid was not seen in our case, but the membrane wall was similar to that of a facet cyst with a communicating channel between the hematoma and the neighboring facet joint.
In conclusion, characteristic MR imaging findings, the posterolateral location to the thecal sac but adjacent to the facet joint, and the direct communication between hematoma and the facet joint, all help make an accurate preoperative diagnosis of a facet cyst hematoma. Prompt recognition of this lesion may allow for definite surgical treatment to prevent irreversible neurological defects.


 XML Download
XML Download