

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
We wanted to evaluate the MDCT findings and concomitant injuries of traumatic adrenal injury in children.
Materials and Methods
Among 375 children who had undergone a MDCT scan for abdominal trauma during the recent five years at our institution, 27 children who had revealed adrenal injury on their CT scan were included in the study. We retrospectively evaluated the causes of the trauma, the patterns of adrenal injury, the associated CT findings and the concomitant injuries of the other organs in the abdomen.
Results
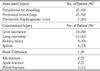
We identified 27 children (7.5%) (17 boys and 10 girls, mean age: 9.9 years, range: 2-18 years) with adrenal injury. The causes of adrenal injury were a traffic accident for 20 patients (74%), falls for four patients (15%) and blunt trauma for three patients (11%). The right adrenal gland was injured in 20 patients (74%), while the left adrenal gland was injured in three patients and bilateral involvement was noted in four patients. The patterns of adrenal injury were round or oval shaped hematoma in 23 lesions (74%), irregular hemorrhage with obliterating the gland in six lesions (19%) and active extravasation of contrast material from the adrenal region in two lesions (7%). Concomitant injuries were noted in 22 patients (81%), including 15 patients with liver laceration (56%), 11 patients with lung contusion (41%) and nine patients with renal injury (33%).
Figures and Tables
Fig. 1
A 7-year-old boy with right adrenal injury caused by blunt trauma.
A. Post contrast axial image shows an ovoid shaped right adrenal hematoma with periadrenal fat stranding (arrow). The image also shows concomitant injury of laceration in caudate lobe of the liver (arrowhead).
B. After 2 months, follow up post contrast axial image demonstrates decreased size of right adrenal hematoma (arrow) and disappeared liver laceration in the caudate lobe.
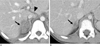
Fig. 2
An 11-year-old boy with right adrenal injury caused by fall down.
Post contrast axial image shows an irregular shaped right adrenal hematoma with periadrenal fat stranding (arrow).
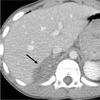
Fig. 3
A 14-year-old boy with right adrenal injury caused by blunt trauma. Post contrast axial image shows extravasated right adrenal hemorrhage.
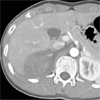
Fig. 4
A 9-year-old boy with right adrenal injury caused by traffic accident.
A. Post contrast axial image shows suspicious low attenuated lesion around right adrenal gland (arrow).
B. Reformatted coronal image reveals small amount of right adrenal hematoma (arrow).

References
1. Rana AI, Kenney PJ, Lockhart ME, McGwin G Jr, Morgan DE, Windham ST 3rd, et al. Adrenal gland hematomas in trauma patients. Radiology. 2004; 230:669–675.
2. Stawichi SP, Hoey BA, Grossman MD, Anderson HL 3rd, Reed JF 3rd. Adrenal gland trauma is associated with high injury severity and mortality. Curr Surg. 2003; 60:431–436.
3. Sivit CJ, Ingram JD, Taylor GA, Bulas DI, Kushner DC, Eichelberger MR. Posttraumatic adrenal hemorrhage in children: CT findings in 34 patients. AJR Am J Roentgenol. 1992; 158:1299–1302.
4. Iuchtman M, Breitgand A. Traumatic adrenal hemorrhage in children: an indicator of visceral injury. Pediatr Surg Int. 2000; 16:586–588.
5. Francque SM, Schwagten VM, Ysebaert DK, Van Marck EA, Beaucourt LA. Bilateral adrenal haemorrhage and acute adrenal insufficiency in a blunt abdominal trauma: a case-report and literature review. Eur J Emerg Med. 2004; 11:164–167.
6. Brengle M, Cohen MD, Katz B. Normal appearance and size of the diaphragmatic crura in children: CT evaluation. Pediatr Radiol. 1996; 26:811–814.
7. Feliciano DV, Mattox KL, Moore EE. Trauma. 6th ed. New York: McGraw-Hill Professional;2008. p. 57–81.
8. Sevitt S. Post-traumatic adrenal apoplexy. J Clin Pathol. 1955; 8:185–194.
9. Pinto A, Scaglione M, Guidi G, Farina R, Acampora C, Romano L. Role of multidetector row computed tomography in the assessment of adrenal gland injuries. Eur J Radiol. 2006; 59:355–358.
10. Burks DW, Mirvis SE, Shanmuganathan K. Acute adrenal injury after blunt abdominal trauma: CT findings. AJR Am J Roentgenol. 1992; 158:503–507.
11. Schwarz M, Horev G, Freud E, Ziv N, Blumenfeld A, Steinberg R, et al. Traumatic adrenal injury in children. Isr Med Assoc J. 2000; 2:132–134.
12. Rammelt S, Mucha D, Amlang M, Zwipp H. Bilateral adrenal hemorrhage in blunt abdominal trauma. J Trauma. 2000; 48:332–335.
13. Sinelnikov AO, Abujudeh HH, Chan D, Novelline RA. CT manifestations of adrenal trauma: experience with 73 cases. Emerg Radiol. 2007; 13:313–318.
14. Murphy BJ, Casillas J, Yrizarry JM. Traumatic adrenal hemorrhage: radiologic findings. Radiology. 1988; 169:701–703.
15. Ikeda O, Urata J, Araki U, Yoshimatsu S, Kume S, Torigoe Y, et al. Acute adrenal hemorrhage after blunt trauma. Abdom Imaging. 2007; 32:248–252.
 XML Download
XML Download