

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Soft tissue tumors and tumor-like lesions of the chest wall are uncommon (1). In addition, hematomas on the thoracic wall are very rare (2), although there have been a few case reports about chronic expanding hematomas in the thorax (234). Yet to the best of our knowledge, a huge, rapidly growing hematoma of the chest wall at the same location as an elastofibroma dorsi has not been previously reported. We describe here a 63-year-old man who was without a history of trauma or a bleeding disorder and who presented with a huge, rapidly growing chest wall hematoma. He had a large mass in his right subscapular space and the computed tomography (CT) and magnetic resonance imaging (MRI) findings were similar to those of elastofibroma dorsi.
Case Report
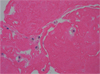
A 63-year-old man presented with a 1-week history of a palpable, rapidly growing, soft tissue mass in his right subscapular region. He had no history of antecedent trauma, tuberculosis or a bleeding disorder. He was a farmer by profession. The physical examination revealed a palpable mass that measured about 10 × 15 cm and was located in the infrascapular area, and this was accompanied by a sensation of heat and tenderness. The laboratory results were within the normal limits. Chest CT analysis showed a right subscapular soft tissue mass of heterogeneous density. The mass had an attenuation value similar to that of the neighboring muscles and there were suspicious linear interspersed hypodense areas, which together with its location suggested a diagnosis of elastofibroma dorsi (Fig. 1). The next day after CT examination, thoracic MRI was performed at a field strength of 1.5 Tesla (Intera; Philips Medical Systems, Best, the Netherlands). MRI analysis showed that the mass was located anterior to the inferior tip of the scapula and between the latissimus dorsi muscle and the ribs of the thoracic cage. The signal intensity was heterogeneous, with most of the mass being of intermediate signal intensity (similar to muscle), including linear high signal foci on the T1-weighted image (T1WI) and mixed high with low signal intensities on the T2-weighted image (T2WI). Moreover, a peripheral dark signal rim on T2WI was associated with this mass. The fat suppressed T2WI showed that this mass was heterogeneously hyperintense. The post-gadolinium enhanced fat suppressed T1WI showed only peripheral rim enhancement without significant internal enhancement of the mass (Fig. 2). The radiologic findings, the location of the mass and the age of the patient suggested a diagnosis of elastofibroma dorsi. The differential diagnosis included hematoma and fibrous tumor (extraabdominal desmoid and fibroma,) as well as hemorrhagic neoplasm such as metastasis and sarcoma. Due to its enlarged size and associated pain, we decided to surgically excise the mass. The operation was done on the fifth day after MRI examination. The patient was placed under general anesthesia, his arm was positioned to expose the mass and a posterolateral incision made over the lesion. The hematoma was loculated and above the latissimus dorsi muscle layer and it was removed. Histologic examination showed a mixture of fibrin, several hemosiderinladen macrophages and blood clots (Fig. 3). Neither elastofibroma nor a fat component was present in the lesion. The patient was finally diagnosed with a chronic hematoma of the chest wall. His postoperative course was uneventful, and he was discharged on the tenth postoperative day. However, he experienced a recurrent hematoma 2 months later and this necessitated re-operation.
Discussion
Chest wall hematoma is rare, and the chest wall hematomas that occur without a history of frank trauma can mimic soft tissue tumors (25). The common soft tissue tumors and non-neoplastic chest wall masses include peripheral nerve tumors, lipomas, liposarcomas, hemangiomas, elastofibromas, lymphomas, metastases from distant tumors, infectious mass lesions, desmoid tumors and malignant fibrous histiocytomas (1). A chest wall mass located anterior to the inferior tip of the scapula and deep in the serratus anterior muscle over the ribs of the thoracic cage can suggest elastofibroma dorsi (67). Imaging examinations are usually performed for patients with chest wall masses to establish a diagnosis and to evaluate the anatomic extension of these masses. The classic MRI signal characteristics of hematomas have been described (5). In a chronic hematoma, the persistence of high signal intensity on T1WI may be caused by recurrent hemorrhage. Continued breakdown of erythrocytes and hemoglobin, with the formation of hemosiderin and the development of fibrosis, may result in foci of distinct low signal intensity. Most hematomas subside without any clinical problems, but a few persist for longer periods of time. Chronic expanding hematoma was first described in 1980 (8) as a persistent hematoma that manifests as an enlarging, space-occupying mass, and this is characterized by persistence and increasing size for more than a month after the initial hemorrhage. This entity may be misdiagnosed as a malignant tumor due to its large size and slowly progressive enlargement. The self-perpetuating expansion of these lesions may be due to the irritant effects of blood and its breakdown products that causes repeated exudation or bleeding from the capillaries in the granulation tissue (9). Chronic expanding thoracic hematoma is quite rare (3), and it usually presents as a slowly expanding mass in patients with histories of either thoracoplasty or tuberculous pleurisy (34). However, our case presented with a huge, rapidly growing thoracic mass, and the patient had no history of tuberculosis, trauma or surgery. Moreover, this mass was located subjacent to the inferior angle of the right scapula area, deep in the serratus anterior muscle and above the latissimus dorsi muscle. Despite being very rare, elastofibroma dorsi that develops in a highly characteristic anatomical location should be considered in the differential diagnosis of a mass in the infrascapular region (6). Elastofibromas are slow growing lesions and their prevalence is relatively high among older individuals that have an occupational history of heavy manual labor (67). Elastofibroma dorsi usually presents as an oval soft tissue mass in the subscapular area, and this area is bordered by the subscapularis, rhomboid, latissimus dorsi and serratus anterior muscles. Elastofibromas are composed of fibrous tissue and on CT, they show heterogeneous soft-tissue attenuation that is generally similar to that of the skeletal muscles, with linear interlaced low density streaks indicative of mature fat. After injection of an iodinated contrast agent, the density of the mass remains virtually unchanged; hence, CT does not provide a definitive diagnosis. MRI shows the alternating pattern of fibrous and fatty tissues, as well as the location of the mass (7). On the STIR sequences, these masses appear as a mosaic of low-intensity and high-intensity areas. The post-gadolinium enhancement has been reported to range from subtle to moderate or marked. The periscapular soft tissue mass lesions that primarily display fibrous tissue generate low signals on T2WI, and these lesions include fibrous tissue tumors (extraabdominal desmoids and fibroma) as well as malignancies such as metastasis and sarcomas. Similarly, the other differential diagnostic options that show increased signal intensity on T1WI include lipoma, liposarcoma, hemangioma and hematoma (67). The MRI findings of chronic expanding hematomas are correlated with their histologic appearances. The central zone that consists of irregularly mixed areas of low and high signal intensity on T2WI correspond histologically to hemosiderin deposition, loose connective tissue, granulation tissue and cavities filled with necrotic debris, fibrin and blood clots. The peripheral rim of low intensity corresponds to the pseudocapsule of hyaline fibrous tissue, whereas the high signal intensity areas on T1WI reflect fresh hemorrhage. The fat suppression sequences show high signals in hematomas, but they show suppressed signals in tumors containing fat (1). Gadolinium-enhanced images can also be used to confirm the identity of the lesion, with an absence of enhancement indicating that the lesion is a hematoma (19). Hematomas may show enhancement, but peripherally this is usually a thin rim (5). A hemorrhagic tumor may be distinguished from a hematoma by the demonstration of tumor nodule or an irregular rim of tumor tissue. An infected or subacute liquefied hematoma may display a similar enhancement pattern and signal characteristics like those of an abscess and so MRI cannot reliably differentiate the former from the latter (10). Yet the mass in the present case contained a subscapular region and it showed heterogeneous signal intensity on T1WI and T2WI, which are findings similar to those of elastofibroma dorsi. A retrospective review showed a heterogeneously hyperintense signal on the fat-suppressed T2WI and a peripheral low signal rim on T2WI, along with peripheral rim enhancement without central enhancement, and these findings differed from those observed in elastofibroma dorsi. The problem of diagnosing this case was that we didn't accurately evaluate whether or not this mass showed fat suppression because of the inhomogeneity of the mass. Therefore, the first diagnosis of this case was elastofibroma dorsi. Pathologic examination of the resected lesion revealed hemosiderin-laden macro-phages with fibrosis, suggesting chronic hematoma. Neither elastofibroma nor a fat component was present in the lesion.
In summary, chronic hematoma of the thorax is a rare condition. Elastofibroma dorsi should be considered in the differential diagnosis of soft tissue tumors located in the infrascapular region, although its incidence is very low. However, a diagnosis of hematoma should be suspected when the mass has T1WI and T2WI signal characteristics of an internal hemorrhage and a peripheral low signal rim, and especially if the lesion does not show central enhancement after gadolinium administration.


 XML Download
XML Download