

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Lipoma arborescens (LA) is a rare intra-articular lesion consisting of villous lipomatous proliferation of the synovium that tends to occur in the knee joint, especially in the suprapatellar pouch (1). The lesion has been observed in other locations, including the glenohumeral joint, subdeltoid bursa, hip, and elbow (2). It may be similar to other proliferations of the synovial membrane, but the characteristic feature is the macroscopic hypertrophic lipomatous synovial tissue. The term "arborescens" describes the characteristic tree-like morphology of this lipomatous villous synovial proliferation, which resembles a frond-like synovial mass (3). Involvement of the hip joint is rarely encountered. To our knowledge, only a few cases were reported. Wolf RS et al. (4) and Noel ER et al. (5) reported hip joint involvement of LA in previous orthopedic and rheumatologic literatures. However, the radiologic literature indicating solitary involvement of the hip joint has not been reported. We report a case of MR imaging on a lipoma arborescens of the hip joint, which was pathologically confirmed. The MRI findings were found to help the early diagnosis of this disorder.
Case Report
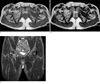
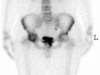
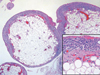
A 34-year-old man presented at our hospital with right hip pain for the last ten years. The symptoms were aggravated after walking. A physical examination revealed no external wound or swelling. Limitation of the right hip motion range was noted and evaluated as follows: (flexion/extension: 100/10, external rotation/internal rotation: 40/10, abduction 30) and the left hip motion range evaluated was as (100/10, 60/40, 60). Vital signs were stable and the white blood count was normal. Plain radiographs showed joint space narrowing and erosive changes in the inferomedial portion of the right femoral head, but no gross calcification (Fig. 1). MRI revealed a large villous, frond-like mass just below the right hip joint, abutting synovium. This synovium-based lesion had a signal intensity similar to that of fat on T1-weighted, T2-weighted, and fat saturated images. Mild joint effusion was noted, but significant marrow edema or erosive changes were not noted (Fig. 2). Whole body bone scan was performed to exclude the possibility of other joint involvement. A radioisotope study noted the increased uptake rate of the right hip joint (Fig. 3). A surgical synovectomy was performed and the microscopic examination of the tumor revealed multiple variable-sized villous masses composed of mature fat tissue and lined by synovial cells (Fig. 4).
Discussion
Synovial lipoma arborescens is a rare disorder of unknown etiology and is characterized by a villolipomatous proliferation of the synovial tissue (3). However, its association with chronic inflammatory disease such as a rheumatoid arthritis, degenerative lesions, or trauma is frequently reported (6). LA is usually mono-articular and mainly localized in the knee, however other articular locations such as the hip (3 cases), the shoulder (2 cases), the wrist (2 cases) and the elbow (1 case) have been described (3). Wolf RS et al. (4) and Noel ER et al. (5) reported hip joint involvement of LA in orthopedic and rheumatologic literatures. Patients typically are seen with a progressive, painless swelling of the joint. As the volume of the effusion increases, pain and limitation of the range of motion often develop. The clinical course is often marked by intermittent exacerbations, with tense effusions lasting for several days (7). The laboratory findings are generally unremarkable and a joint fluid study was negative for crystal or bacterial infection (8). The appearance of LA on MRI is believed to be pathognomonic. MRI outlined the synovial mass and readily revealed its frond-like appearance. The lesion demonstrated the same signal intensity as fat on all sequences (7). In this case, we could see a large villous, frond-like mass just below right hip joint abutting the synovium. The signal of the lesion was similar to that of fat on T1-weighted, T2-weighted, and fat saturated images. The differential diagnosis of LA includes intra-articular lipoma, synoval hemangioma, and chronic inflammatory synovial proliferation. Intra-articular lipoma is a solitary localized mass of adipose tissue with a round or oval contour without synovial changes, whereas LA is characterized by diffuse subsynovial fat deposition of a villous appearance, associated joint effusion, and a synovial cyst (2). However, precise differentiation lies in the microscopic and macroscopic appearances. Under the microscope, LA revealed diffuse replacement of the subsynovial layer by mature fat cells with moderate infiltration of mononuclear inflammatory cells. Intra-articular lipomas, which may be covered by the synovium, does not arise from or replace the subsynovial layer (9). Synovial hemangiomas appear as intra-articular or extra-articular lesions of intermediate signal intensity on T1- and T2-weighted images, with areas of low signal intensity corresponding to calcified phleboliths or a fluid void in abnormal vessels (2). In this case, clinical diagnosis was synovitis but we could diagnose it as LA because of the characteristic shape of the villous, frond-like mass, which had similar signals to fat. The recommended treatment for LA is arthrotomy and synovectomy (10).
We report MR findings of a case of lipoma arborescens of the unilateral hip joint, which is a rare intra-articular lesion that should be considered in the differential diagnosis of patients who have joint swelling. MRI allows a specific preoperative diagnosis and differential diagnosis.

 XML Download
XML Download