

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
We wanted to evaluate the incidence and clinical features of perifissural air seen in the pneumomediastinum on CT.
Materials and Methods
The study included the CT scans of 90 patients with pneumomediastinum (65 males and 25 females) and who had been treated during the recent 3 years. The ages ranged from 2 to 48 years (mean age: 41 years). The patients were divided into 3 groups, I: perifissural air (n=7), II: pneumomediastinum without perifissural air (n=83) and III: pulmonary interstitial emphysema involving the peribronchial or intraparenchymal area (n=9) of the Group II. We analyzed the clinical data and compared it between group I and the other groups.
Results
Group I included 7.8% of the total cases. Age was statistically different between Group I and II, but age was not significantly different between Groups I and III (I: 13.7 years, II: 42.9, III: 26.4). A spontaneous cause was the most common (57.2%) in Group I, trauma (33.7%), postoperative occurrence (20.5%) and a spontaneous cause (9.7%) were common in Group II, and trauma (44.4%) and a spontaneous cause (33.3%) were common in Group III. The incidence of a spontaneous cause was statistically different between Groups I and II (p<0.001), but this was not significantly different between Groups I and III.
Figures and Tables
Fig. 1
Perifissural air in a 16-year-old boy (Group I).
He did not have the any history of trauma and operation, and underlying disorders, so the cause of pneumomediastinum is classified as spontaneous.
A. Reformatted sagittal view shows air collection with internal linear structures near the minor fissure (arrow) and major fissure (arrowhead) in the right lung.
B. Coronal view shows abnormal air collection (arrow) near the interlobar fissure. Also seen pneumomediastinum.
C. Axial view shows abnormal air collection with internal linear and nodular structures near the minor fissure (arrow) and major fissure (arrowhead).
The internal linear and nodular structures in the air collection are suggestive of subpleural interstitial connective tissues. Outer margin of perifissural air is not smooth. These findings are differential diagnostic points from pneumothorax of interlobar fissure.
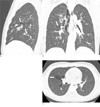
Fig. 2
Perifissural air caused by spontaneous cause in a 16-year-old boy (Group I).
Axial scan shows localized air collection with internal linear structures (arrow) near the left major fissure.

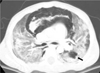
Fig. 3
Peribronchial air caused by stab injury in a 21-year-old woman with pneumomediastinum and pneumothorax (Group III).
Axial scan shows interstitial free air collections along left lower bronchus (arrow head) and along segmental artery and vein (arrow) of left lower lobe. These findings reveal Macklin effect on CT.



References
1. Wood BP, Anderson VM, Mauk JE, Merritt TA. Pulmonary lymphatic air: locating "pulmonary interstitial emphysema" of the premature infant. AJR Am J Roentgenol. 1982; 138:809–814.
2. Macia I, Moya J, Ramos R, Morera R, Escobar I, Saumench J, et al. Spontaneous pneumomediastinum: 41 cases. Eur J Cardiothorac Surg. 2007; 31:1110–1114.
3. deRoux SJ, Prendergast NC. Large sub-pleural air cysts: an extreme form of pulmonary interstitial emphysema. Pediatr Radiol. 1998; 28:981–983.
4. Campbell RE. Intrapulmonary interstitial emphysema: a complication of hyaline membrane disease. Am J Roentgenol Radium Ther Nucl Med. 1970; 110:449–456.
5. Macklin CC. Transport of air along sheaths of pulmonic blood vessels from alveoli to mediastinum: clinical implications. Arch Intern Med. 1939; 64:913–926.
6. Wintermark M, Wicky S, Schnyder P, Capasso P. Blunt traumatic pneumomedistinum: using CT to reaveal the Macklin effect. AJR Am J Roentgenol. 1999; 172:129–130.
7. Albelda SM, Gefter WB, Kelley MA, Epstein DM, Miller WT. Ventilator-induced subpleural air cysts: clinical, radiographic, and pathologic significance. Am Rev Respir Dis. 1983; 127:360–365.
8. Zylak CM, Standen JR, Barnes GR, Zylak CJ. Pneumomediastinum revisited. Radiographics. 2000; 20:1043–1057.
9. Trotman-Dickenson B. Radiology in the intensive care unit (part 2). J Intensive Care Med. 2003; 18:239–252.
10. Demura Y, Ishizaki T, Nakanishi M, Ameshima S, Itoh H. Persistent diffuse pulmonary interstitial emphysema mimicking pulmonary emphysema. Thorax. 2007; 62:652.
11. Bertolini G, Stefanello C, Caldin M. Imaging diagnosis--pulmonary interstitial emphysema in a dog. Vet Radiol Ultrasound. 2009; 50:80–82.
12. Oh MH, Kim MY, Shim WS, Oh SS, Shin BK, Cho SJ, et al. A case of localized persistent interstitial pulmonary emphysema. J Korean Med Sci. 2001; 16:225–228.
13. Bullaro FM, Bartoletti SC. Spontaneous pneumomediastinum in children: a literature review. Pediatr Emerg Care. 2007; 23:28–30.
14. Damore DT, Dayan PS. Medical causes of pneumomediastinum in children. Clin Pediatr (Phila). 2001; 40:87–89.
 XML Download
XML Download