

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Adrenal rest tumors are aberrant adrenocortical tissue which has been most commonly described in abdominal and pelvic sites. To our knowledge, there has been no previous description of an adrenal rest tumor of the greater omentum. We present a case of a pathologically confirmed adrenal rest tumor of the greater omentum in a 76-year-old man.
Figures and Tables
Fig. 1
76-year-old man with adrenal rest tumor of the greater omentum.
A. Contrast-enhanced CT scan obtained during portal phase shows heterogeneous enhancing mass (arrow), seems to adhere to gastric wall.
B. Mass (arrow) abuts the gastric fundus wall in coronal image.


Fig. 3
76-year-old man with adrenal rest tumor of the greater omentum.
A. Contrast-enhanced CT scan obtained during arterial phase shows feeding vessel (arrow) branched from left hepatic artery.
B. Sagittal image shows feeding vessel (arrow) and mass (M) abuting the gastric wall.

Fig. 4
76-year-old man with ruptured adrenal rest tumor of the greater omentum.
Contrast-enhanced CT scan shows obscured boundary of mass around fundus of stomach and abundant hyperattenuated fluid in peritoneum.
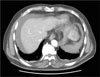
Fig. 5
76-year-old man with adrenal rest tumor of the greater omentum.
A. The microscopic picture of the tumor shows proliferation of large polygonal cells with abundant eosinophilic cytoplasms and atypical nuclei. The tumor cells are arranged around the slit like sinusoidal vessels without fibrosis (Original magnification, ×200 Hematoxylin & Eosin stain).
B. Electron micrograph from paraffin embedded tissue of the tumor (Original magnification, ×5000 uranyl acetate-lead citrate stain). Multiple oval to round mitochondria with electron dense inclusions in the cytoplasm (arrow) suggest that the tumor cells are originated in adrenal gland (M: mitochondria, N: nucleus, L: lipid vacuole).

References
1. Schechter DC. Aberrant adrenal tissue. Ann Surg. 1968; 167:421–425.
2. Bothe AE. Hypernephromata. Ann Surg. 1926; 84:57–88.
3. Bozic C. Ectopic fetal adrenal cortex in the lung of a newborn. Virchows Arch Path Anat. 1974; 363:371–374.
4. Weiner MF, Dallgaard SA. Intracranial adrenal gland: a case report. Arch Pathol. 1959; 67:228–233.
5. McLetchie NGB, Scott LDW. Carcinoma of an adreno-cortical rest associated with hypophyseal abnormality. J Endocrinol. 1942; 3:347–355.
6. Tajima T, Funakoshi A, Ikeda Y, Hachitanda Y, Yamaguchi M, Yokota M, et al. Nonfunctioning adrenal rest tumor of the liver : radiologic appearance. J Comput Assist Tomogr. 2001; 25:98–101.
7. Baba Y, Beppu T, Imai K, Masuda T, Iyama K, Sasano H, et al. A case of adrenal rest tumor of the liver: radiological imaging and immunohistochemical study of steroidogenic enzymes. Hepatol Res. 2008; 38:1154–1158.
8. Macmillan SF, Gilbert JB. Aberrant adrenal tumor of upper part of abdomen. Arch Surg. 1940; 40:77–82.
9. Nicholson BS. Abnormal position of suprarenal gland. Br Med J. 1894; 1:408.
 XML Download
XML Download