

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To determine the optimal skin site for retrograde common femoral arterial puncture based on the inguinal skin crease.
Materials and Methods
We retrospectively evaluated CT arteriographic images of right groins in 200 patients. We measured the relative distances of the common femoral artery bifurcation and inguinal ligament from the inguinal skin crease, respectively. We calculated the rates of common femoral artery puncture at 1 mm intervals, above or below the inguinal skin crease.
Results
The range in skin site where the rates of common femoral artery puncture were greater than 60%, 70%, and 80% were situated between 3 mm below to 27 mm above, 1 mm to 23 mm above, and 5 mm to 15 mm above the inguinal skin crease, respectively. The skin site of the highest puncture rate was 10 mm above inguinal skin crease (85.2%).
Figures and Tables
Fig. 1
Three-dimensional images of inguinal skin crease (ISC) and femoral artery
A. A volume-rendering image shows the ISC at anteroposterior
projection.
B. A volume-rendering images shows the measurement methods
of reference intersecting points (A, B, C) and horizontal lines
(A, B, C) at anteroposterior view.
A thick oblique line means ISC and a dotted oblique line means
inguinal ligament (IL).
Point A: intersecting point between inguinal ligament and
femoral artery,
Point B: CFA bifurcation,
Point C: intersecting point between inguinal skin crease and
femoral artery,
Line A: horizontal line, passing Point A,
Line B: horizontal line, passing Point B (CFA bifurcation),
Line C: horizontal line, passing Point C,
C. The CFA and re-established skin puncture site on a sagittal view
Point A`= Point A - skin depth of Point A
Point B`= Point B - skin depth of Point B

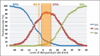
Fig. 2
The Graph shows the arterial puncture rate at each distance above or below the inguinal skin crease (SC). The distance with the highest percentage of common femoral artery (CFA) puncture rate was 10 mm above the inguinal skin crease in 85.2% of the cases. The ranges of optimal skin site for retrograde common femoral arterial puncture rates of more than 60%, 70% and 80% of CFA puncture rate was from 3 mm below to 27 mm above, from 1 mm to 23 mm above, and from 5 mm to 15 mm above, respectively.
(SFA : superficial femoral artery, EIA : external iliac artery)

References
1. Millward SF, Burbridge BE, Luna G. Puncturing the pulseless femoral artery: a simple technique that uses palpation of anatomic landmarks. J Vasc Interv Radiol. 1993; 4:415–417.
2. Grier D, Hartnell G. Percutaneous femoral artery puncture: practice and anatomy. Br J Radiol. 1990; 63:602–604.
3. Dotter CT, Rosch J, Robinson M. Fluoroscopic guidance in femoral artery puncture. Radiology. 1978; 127:266–267.
4. Garrett PD, Eckart RE, Bauch TD, Thompson CM, Stajduhar KC. Fluoroscopic localization of the femoral head as a landmark for common femoral artery cannulation. Catheter Cardiovasc Interv. 2005; 65:205–207.
5. Lechner G, Jantsch H, Waneck R, Kretschmer G. The relationship between the common femoral artery, the inguinal crease, and the inguinal ligament: a guide to accurate angiographic puncture. Cardiovasc Intervent Radiol. 1988; 11:165–169.
6. Schnyder G, Sawhney N, Whisenant B, Tsimikas S, Turi ZG. Common femoral artery anatomy is influenced by demographics and comorbidity: implications for cardiac and peripheral invasive studies. Catheter Cardiovasc Interv. 2001; 53:289–295.
7. Grossman M. How to miss the profunda femoris. Radiology. 1974; 111:482.
8. Yeow KM, Toh CH, Wu CH, Lee RY, Hsieh HC, Liau CT, et al. Sonographically guided antegrade common femoral artery access. J Ultrasound Med. 2002; 21:1413–1416.
9. Hessel SJ, Adams DF, Abrams HL. Complications of angiography. Radiology. 1981; 138:273–281.
10. Rapoport S, Sniderman KW, Morse SS, Proto MH, Ross GR. Pseudoaneurysm: a complication of faulty technique in femoral arterial puncture. Radiology. 1985; 154:529–530.
11. Illescas FF, Baker ME, McCann R, Cohan RH, Silverman PM, Dunnick NR. CT evaluation of retroperitoneal hemorrhage associated with femoral arteriography. AJR Am J Roentgenol. 1986; 146:1289–1292.
12. Rupp SB, Vogelzang RL, Nemcek AA Jr, Yungbluth MM. Relationship of the inguinal ligament to pelvic radiographic landmarks: anatomic correlation and its role in femoral arteriography. J Vasc Interv Radiol. 1993; 4:409–441.
13. Spector KS, Lawson WE. Optimizing safe femoral access during cardiac catheterization. Catheter Cardiovasc Interv. 2001; 53:209–212.
14. Chung HH, Ha JS, Cha SH, Kim BH, Lee KY, Kim TK, Lee SH, Kim JH, Seol HY. Femoral Arterial Puncture: Comparison of Using the Inguinal Crease and Bony Landmarks. J Korean Radiol Soc. 2006; 54:251–257.
15. Jeon MH, Han GS, Kim SJ, Park KS, Cha SH, Bae IH, Lee SY. Anatomic Landmarks of Fluoroscopy Guided Puncture of the Pulseless Femoral Artery. J Korean Radiol Soc. 2006; 55:53–57.
16. Spijkerboer AM, Scholten FG, Mali WP, van Schaik JP. Antegrade puncture of the femoral artery: morphologic study. Radiology. 1990; 176:57–60.
 XML Download
XML Download