

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The aim of this study was to evaluate the chest CT features of nontuberculous mycobacterial (NTM) disease regardless of the specific organisms.
Materials and Methods
This study included 74 consecutive patients (35 men, 39 women; mean age, 63 years; age range, 25-89 years) who were diagnosed with NTM disease according to the American Thoracic Society Guidelines (1997 and 2007) between January 2005 and July 2007. Chest CT images were randomly reviewed by two radiologists with consensus.
Results
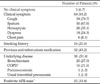
The most common organism associated with NTM disease is M. avium-intracellulare complex (87.8%), followed by M. abscessus, M. kansasii, and M. chelonae. The most common chest CT finding was a nodular bronchiectatic lesion (n = 35, 46.7%), followed by a cavitary lesion of the upper lobe (n = 21, 28.0%), combined lesions of two prior subtypes (n = 6, 8.0%), consolidative lesion (s) (n = 5, 6.7%), a bronchogenic spreading pulmonary tuberculosis-like lesion (n = 5, 6.7%), a cavitary mass lesion with small satellite nodules (n = 2, 2.7%), and a miliary nodular lesion (n = 1, 1.3%). More than 5 segments were involved in 60 cases (81.1%).
Figures and Tables
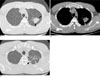
 | Fig. 1A 68-year-old woman with hemoptysis. Cultures from bronchoalveolar lavage fluid showed Mycobacterium avium-intracellulare complex.A, B. axial CT images at the level of mid-thorax show multiple tubular bronchiectasis with multiple centrilobular nodules and branching linear structures (white arrows) in both lungs. These findings are typical findings of nodular bronchiectatic form of pulmonary NTM disease. Also there are peribronchial consolidations with mild volume loss (black arrows) in right middle lobe and inferior lingular segment of left upper lobe.
|
 | Fig. 2A 72-year-old man with chest pain. Cultures from sputum showed Mycobacterium avium-intracellulare complex.A, B (lung window setting) and C, D (mediastinal window setting), axial continuous CT images at levels of upper thorax show cavitary consolidations (white arrows) with perilesional fibrocicatrization in left upper lobe. These findings are typical findings of upper lobe cavitary form of pulmonary NTM disease. Also old inflammatory lesions (black arrows) are seen in right upper lobe.
|
 | Fig. 3A 34-year-old woman without any respiratory symptoms. Cultures from bronchoalveolar lavage showed Mycobacterium avium-intracellulare complex.A, B. axial CT images at the level of mid-thorax show only a focal nodular consolidation (white arrows) in lingular segment of left upper lobe.
|
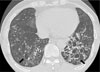
 | Fig. 4A 77-year-old woman with cough and sputum. Cultures from sputum showed Mycobacterium avium-intracellulare complex.A, B. axial CT images at the level of mid-to-lower thorax show multiple air-space nodules and branching linear structures (white arrows) in both lungs with a cavitary nodule (black arrow) in right lower lobe.
|
 | Fig. 5A 44-year-old man with productive cough and hemoptysis. Cultures from sputum showed Mycobacterium avium-intracellulare complex.A, B. axial CT images at the level of upper thorax show a 3.2 cm cavitary mass (arrows) containing stippled calcific foci in left apical lung.
C. axial CT image, obtained at more cranial level than A, B. shows multiple satellite nodules (arrowhead) in surrounding lung parenchyma
|
 | Fig. 659-year-old man with dyspnea and hemoptysis. Cultures from sputum showed Mycobacterium kansasii. Axial CT image at the level of lower thorax shows multiple cystic bronchiectasis with bronchial wall thickening, mucoid impactions and air-fluid levels (arrows) in both lungs.
|


References
1. Diagnosis and. This official statement of the American Thoracic Society was approved by the Board of Directors, March 1997. Medical Section of the American Lung Association. Am J Respir Crit Care Med. 1997; 156:S1–S2.
2. Management of. Joint tuberculosis committee guidelines 1999. Subcommittee of the joint tuberculosis committee of the british thoracic society. Thorax. 2000; 55:210–221.
3. Wolinsky E. Nontuberculous mycobacteria and associated diseases. Am Rev Respir Dis. 1979; 119:107–159.
4. Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007; 175:367–416.
5. Erasmus JJ, McAdams HP, Farrell MA, Patz EF Jr. Pulmonary nontuberculous mycobacterial infection: radiologic manifestations. Radiographics. 1999; 19:1487–1505.
6. Martinez S, McAdams HP, Batchu CS. The many faces of pulmonary nontuberculous mycobacterial infection. AJR Am J Roentgenol. 2007; 189:177–186.
7. Ellis SM. The spectrum of tuberculosis and non-tuberculous mycobacterial infection. Eur Radiol. 2004; 14:Suppl 3. E34–E42.
8. Koh WJ, Kwon OJ, Lee KS. Nontuberculous mycobacterial pulmonary diseases in immunocompetent patients. Korean J Radiol. 2002; 3:145–157.
9. Kwon YS, Koh WJ, Chung MP, Kwon OJ, Lee NY, Cho EY, et al. Solitary pulmonary nodule due to Mycobacterium intracellulare: the first case in Korea. Yonsei Med J. 2007; 48:127–130.
10. Bai GH, Park KS, Kim SJ. Clinically isolated mycobacteria other than Mycobacterium tuberculosis from 1980 to 1990 in Korea. J Korean Soc Microbiol. 1993; 28:1–5.
11. Yoon CJ, Goo JM, Seo JB, Kim SH, Im JG. CT findings of mycobacterial infection other than tuberculosis: comparison with tuberculosis. J Korean Radiol Soc. 2000; 42:487–492.
12. Lew WJ, Ahh DI, Yoon YJ, Cho JS, Kwon DW, Kim SJ, et al. Clinical experience of mycobacterial disease other than tuberculosis. Tuberc Respir Dis. 1992; 39:425–432.
13. Christensen EE, Dietz GW, Ahn CH, Champman JS, Murry RC, Adnerson J, et al. Initial roentgenographic manifestations of pulmonary Mycobacterium tuberculosis, M kansasii, and M intracellularis infections. Chest. 1981; 80:132–136.
14. Koh WJ, Lee KS, Kwon OJ, Jeong YJ, Kwak SH, Kim TS. Bilateral bronchiectasis and bronchiolitis at thin-section CT: diagnostic implications in nontuberculous mycobacterial pulmonary infection. Radiology. 2005; 235:282–288.
15. Chung MJ, Lee KS, Koh WJ, Lee JH, Kim TS, Kwon OJ, et al. Thinsection CT findings of nontuberculous mycobacterial pulmonary diseases: comparison between Mycobacterium avium-intracellulare complex and Mycobacterium abscessus infection. J Korean Med Sci. 2005; 20:777–783.
 XML Download
XML Download