

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The aim of this study is to determine the causes of acute cholangitis without the biliary obstruction and radiological findings.
Materials and Methods
This study was performed retrospectively. A total of 135 patients diagnosed with acute cholangitis in a clinical setting based on the review of the radiologic findings from an ultrasonogram (USG), computed tomogram (CT), or magnetic resonance images (MRI). Among them, patients with a biliary obstruction as a result of a stone, tumor, lymph node, stricture were excluded. A total of 31 patients had acute cholangitis without a definite biliary obstruction. We analyzed their causes and imaging features with the USG and CT image.
Results
The causes of acute cholangitis without biliary obstruction included Clonorchis sinensis cholangitis in 15 cases (48%), post-operative swelling after gastrojejunostomy, pylorus preserved partial duodenectomy, and choledochojejunostomy in 7 cases (22.6%), recent spontaneous passage of a distal CBD stone in 3 cases (9.7%), compression effect by the large duodenal diverticulum in 2 cases (6.5%), and unknown causes in 4 cases (12.9%).
Figures and Tables
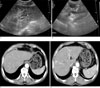 | Fig. 168-year-old man with mild infestation of clonorchis sinensis.A. Transverse scan of left hepatic lobe shows severe dilatation of bile ducts with echogenic bands (between arrows) along dilated bile ducts, indicating severe fibrous thickening of wall.
B. The common bile duct is not specific (arrow).
C, D. CT scan shows diffuse mild uniform dilatation in both peripheral intrahepatic ducts and periductal fibrous tissue is enhanced (arrows).
|
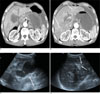 | Fig. 2Acute suppurative cholangitis caused by duodenal reflux after Billroth type I anastomosis in a 72-year-old man with abdominal pain, a high fever, and jaundice.A, B. Contrast-enhanced CT images show profound dilatation of bile ducts with periductal (arrows) and pericapsular (arrowhead) enhancement.
C. Transverse ultrasonogram shows diffuse hyperechoic thickening of the gallbladder wall-a finding indicative of acute inflammation (arrow).
D. Both intrahepatic ducts show also diffuse dilatated with hyperechoic thickening (arrows).
|
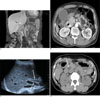 | Fig. 343-year-old woman with epigastric pain.A. Coronal reformated contrast-enhanced fat-suppressed T1-weighted image shows mild dilatation in common bile duct with wall thickening and enhancement (arrow).
B. Abnormal mass or stone is not noted in distal common bile duct.
C. In ultrasound, common bile duct shows wall thickening at transverse scan (arrows).
D. 2 days ago, axial non-contrast CT scan checked in local clinic shows small calcified stone (arrow) in distal common bile duct
|
 | Fig. 4Acute suppurative cholangitis caused by duodenal diverticulum in a 70-year-old man with abdominal pain, a high fever, and jaundiceA, B. Axial contrast enhanced fat-suppressed T1-weighted images show mild dilatated both intrahepatic ducts (arrow) and common bile duct with wall thickening (arrowhead) and periductal prominent enhancement.
C, D. At distal common bile duct level, large air filled duodenal diverticulum (arrow) is noted with indent distal common bile duct (arrowhead). His symptom was relieved after diverticulectomy.
|




References
1. Yasuda H, Takada T, Kawarada Y, Nimura Y, Hirata K, Kimura Y, et al. Unusual cases of acute cholecystitis and cholangitis: Tokyo Guidelines. J Hepatobiliary Pancreat Surg. 2007; 14:98–113.
2. Zandrino F, Benzi L, Ferretti ML, Ferrando R, Reggiani G, Musante F. Multislice CT cholangiography without biliary contrast agent: technique and initial clinical results in the assessment of patients with biliary obstruction. Eur Radiol. 2002; 12:1155–1161.
3. Zandrino F, Curone P, Benzi L, Ferretti ML, Musante F. MR versus multislice CT cholangiography in evaluating patients with obstruction of the biliary tract. Abdom Imaging. 2005; 30:77–85.
4. Denecke T, Degutyte E, Stelter L, Lehmkuhl L, Valencia R, Lopez-Hänninen E, et al. Minimum intensity projections of the biliary system using 16-channel multidetector computed tomography in patients with biliary obstruction: comparison with MRCP. Eur Radiol. 2006; 16:1719–1726.
5. Anderson SW, Rho E, Soto JA. Detection of biliary duct narrowing and choledocholithiasis: accuracy of portal venous phase multidetector CT. Radiology. 2008; 247:418–427.
6. Wada K, Takada T, Kawarada Y, Nimura Y, Miura F, Yoshida M, et al. Diagnostic criteria and severity assessment of acute cholangitis: Tokyo Guidelines. J Hepatobiliary Pancreat Surg. 2007; 14:52–58.
7. Hou PC. The pathology of clonorchis sinensis infestation of the liver. J Pathol Bacteriol. 1955; 70:53–64.
8. Lim JH. Radiologic findings of clonorchiasis. AJR Am J Roentgenol. 1990; 155:1001–1008.
9. Lim JH, Kim SY, Park CM. Parasitic diseases of the biliary tract. AJR Am J Roentgenol. 2007; 188:1596–1603.
10. Lim JH, Mairiang E, Ahn GH. Biliary parasitic diseases including clonorchiasis, opisthorchiasis and fascioliasis. Abdom Imaging. 2008; 33:157–165.
11. Blankenstein JD, Terpstra OT. Early and late results following choledochoduodenostomy and choledochojejunostomy. HPB Surg. 1990; 2:151–158.
12. Panis Y, Fagniez PL, Brisset D, Lacaine F, Levard H, Hay JM. Long term results of choledochoduodenostomy versus choledochojejunostomy for choledocholithiasis. The french associatiation for surgical research. Surg Gynecol Obstet. 1993; 177:33–37.
13. Bismuth H, Franco D, Corlette MB, Hepp J. Long term result of Roux-en-Y hepaticojejunostomy. Surg Gynecol Obstet. 1978; 146:161–167.
14. McKee JD, Raju GP, Edelman RR, Levine H, Steer M, Chuttani R. MR cholangiopancreatography (MRCP) in diagnosis of afferent loop syndrome presenting as cholangitis. Dig Dis Sci. 1997; 42:2082–2086.
15. Matthews JB, Baer HU, Schweizer WP, Gertsch P, Carrel T, Blumgart LH. Recurrent cholangitis with and without anastomotic stricture after biliary-enteric bypass. Arch Surg. 1993; 128:269–272.
16. Tranter SE, Thompson MH. Spontaneous passage of bile duct stones: frequency of occurrence and relation to clinical presentation. Ann R Coll Surg Engl. 2003; 85:174–177.
17. Sakai Y, Tsuyuguchi T, Ishihara T, Yukisawa S, Ohara T, Tsuboi M, et al. Is ERCP really necessary in case of suspected spontaneous passage of bile duct stones? World J Gastroenterol. 2009; 15:3283–3287.
18. Sakai Y, Tsuyuguchi T, Yukisawa S, Tsuchiya S, Sugiyama H, Miyakawa K, et al. Diagnostic value of magnetic resonance cholangiopancreatography for clinically suspicious spontaneous passage of bile duct stones. J Gastroenterol Hepatol. 2008; 23:736–740.
19. Nande AG. Spontaneous passage of large common bile duct calculus. Am J Gastroenterol. 1989; 84:1465.
20. Saranovic D, Djuric-Stefanovic A, Milovanovic A, Kratovac-Dunjic M, Masulovic D, Ivanovic A. Education and imaging. Hepatobiliary and pancreatic: juxtapapillary duodenal diverticulum causing cholestasis. J Gastroenterol Hepatol. 2009; 24:496.
21. Kim JG, Oh JY, Cho JH, Kwon HJ, Nam KJ, Kim MC. The Relationship between Juxtapapillary Duodenal Diverticula and Biliary Diseases: An Evaluation by the Use of MDCT Multiplanar Reformation. J Korean Radiol Soc. 2008; 59:183–189.
 XML Download
XML Download