

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A desmoid tumor of the breast is a rare, locally aggressive disease (1). An accurate diagnosis is difficult because of the similar clinical and imaging findings to a breast malignancy. Desmoid tumors are found mainly in young women and in patients with previous surgical trauma or reconstruction. We report the case of a 72-year-old female presenting with an aggressive desmoid tumor that mimicked breast carcinoma but was not associated with previous trauma history.
Case Report
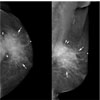
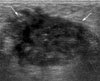
A 72-year-old woman presented with a palpable mass with four months duration in the outer portion of her left breast. She had no prior history of breast problems and no family history of breast cancer. In addition, she had no history of breast augmentation or other breast surgery. She also had no prior history of hormone replacement therapy. The clinical breast examination revealed an 8.0-cm long, firm, non-tender mass in the 3 o'clock position with overlying skin retraction. The mass was fixed to the chest wall. There was no evidence of axillary or supraclavicular adenopathy. Mammography (Fig. 1) revealed an ill-defined, irregular shaped, hyperdense mass that appeared to involve the pectoral muscle in the upper outer quadrant of her left breast. The ultrasound images (Fig. 2) showed a 4.0-cm in length irregular hypoechoic mass with an ill-defined margin located in the 3 o'clock position and approximately 0.5 cm from the nipple. Power Doppler sonography revealed increased vascularity around the mass. This lesion was thought to be highly suspicious for a malignancy and was classified as Breast Imaging Reporting and Data System (BI-RADS) category 5.
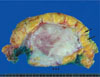
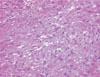
A 14-gauge core needle biopsy was performed with ultrasound guidance. The microscopic evaluation revealed spindle cells and collagen fibers without a malignant component. As the pathologic findings were not concordant with the imaging findings, the patient underwent a surgical excision to obtain a definitive diagnosis. A gross pathological evaluation of the specimen (Fig. 3), revealed a 7.5×6.5×5-cm long, pinkish-white, fibrotic mass with an irregular shape and an ill-defined margin involving the breast parenchyma and pectoralis major muscle. The microscopic evaluation (Fig. 4) revealed spindle cells interlacing bundles and fascicles with collagen fibers. Spindle cells infiltrated both pectoral muscles and breast parenchyma (Figs. 5A, B). However, the spindle cells were uniform showing no mitotic activity. The final pathologic diagnosis was a desmoid tumor.
DISCUSSION
A desmoid tumor arising in the breast, which is also referred to as low-grade fibrosarcoma and aggressive fibromatosis, is an rare lesion marked by infiltrating, histologically low-grade spindle cell proliferation (1). Desmoid tumors arise primarily within the breast tissue or from the aponeurotic fascia or pectoralis muscle, and often infiltrate into the surrounding fat and glandular parenchyma. It frequently recurs after an excision due to its infiltrating features but lacks metastatic potential(1).
Desmoid tumors comprise 0.2% of all breast tumors and 0.3% of all solid tumors (2). The average tumor size ranges from 2.5 cm to 3.0 cm in length. The patients' age ranges from 13 to 83 years, but the mean age at diagnosis ranges from 37 to 50.3 years of age (13).
The etiology of a desmoid tumor is unknown. Associations with surgical trauma, familial desmoid and Gardner's syndromes, hormonal influence, and saline or silicone implants have been reported (4). Many reports revealed desmoid development after surgical trauma and breast reconstruction. Some of these reports suggest that the tumor has arisen from the fibrous capsule placement of breast implants (25). There may be a hormonal influence because desmoid tumors are more prevalent in females than in males and may initially develop or grow during pregnancy (5).
Most cases of desmoid tumors in the breast present with a mobile, firm, typically painless mass. Skin and nipple retraction might be present but there is no adenopathy (1). Mammography shows a typically malignant mass, such as a spiculated, high-density mass. Ultrasound often shows irregular hypoechoic masses. Therefore, this tumor is clinically, mammographically and sonographically interpreted as being suspicious for a malignancy. MRI shows isointense masses on the T1-weighted images and lower or high intensity lesions on the T2-weighted images with heterogeneous and gradual enhancement (6). As the enhancing pattern is not typical for breast cancer, it can also help in distinguishing between malignant and benign breast tumors.
Histopathologically, this lesion is composed of spindle cells with a variable amount of collagen and rarely shows nuclear atypia or pleomorphism (7). Therefore, a core biopsy or FNA often shows benign fibrosis or inconclusive findings (1). The differential diagnoses include malignant lesions, such as metaplastic carcinoma, high-grade fibrosarcoma and fibrous histiocytoma, as well as benign conditions, such as nodular fasciitis, benign phyllodes and a radial scar (8).
The treatment of choice is surgical excision with side margins. Complete excision of the mass along with all affected skin, muscle, and fascia is required because the margin status has been associated with a high recurrence rate (29%) (57). The relatively high recurrence rate has led to research on many adjuvant treatments, including radiation therapy, and many pharmacologic therapy, including nonsteroidal anti-inflammatory drugs (NSAIDs), hormonal agents, and cytotoxic therapy (9). However, none has been proven effective due to the rarity of the disease.
We report a case of mammary desmoid tumor that mimicked breast carcinoma in an older woman with no history of breast surgery. Although a mammary desmoid tumor is rare, it should be included in a differential diagnosis when the image of a malignant-appearing mass adjacent to the chest wall does not correlate with the pathology results.

 XML Download
XML Download