

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A ciliated foregut cyst is an uncommon developmental anomaly expressed as bronchial or esophageal cysts and usually develops above the diaphragm, however on rare occasions, does occur below the diaphragm (1). Ciliated cysts are considered benign, but are radiologically difficult to differentiate from a malignant neoplasm, which is a cystic structure in or adjacent to the gallbladder (2). To our knowledge, only a few cases of gallbladder cysts that are lined by a ciliated epithelium have been reported (12345), and no ciliated foregut cyst of the gallbladder has been described in the radiologic literature. We report a case of a ciliated foregut cyst arising from the gallbladder with its imaging findings in an asymptomatic 63-year-old man.
Case Report
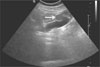
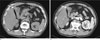
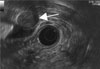
A 63-year-old man was referred to our hospital after a screening US revealed a tumor in the gallbladder. He had not experienced any abdominal symptoms or demonstrable abnormality in laboratory findings. An abdominal US revealed a 2.2-cm, well-demarcated hypoechoic mass with posterior enhancement and internal hyperechoic content in the gallbladder wall (Fig. 1). It was shown to be unilocular without mural nodules. An abdominal CT revealed that the cystic lesion showed a non-enhancing round soft tissue mass with high attenuation in the gallbladder wall, which was lined by enhancing intact mucosal layer (Figs. 2A, B). An endoscopic ultrasonography (EUS) also showed a 2.2-cm well-delineated round hypoechoic mass that originated from the gallbladder wall (Fig. 3).
The potential for malignancy could not be ruled out by abdominal US, EUS, and CT. Thus, complete excision of the gallbladder was performed by a laparoscopic cholecystectomy. The tumor was 2.0 cm in diameter with a smooth external surface and the gallbladder was found to be in normal position.
Grossly, there was a subserosal cystic mass measuring 2.0×1.5 cm, filled with a milky fluid admixed with the horny debris. The mucosa was velvety without nodule or mass. Moreover, neither communication with the lumen of the gallbladder nor stones were found.
Microscopically, the cyst was located in the serosal area of the gallbladder (Fig. 4A). The cyst was found to be lined by ciliated, pseudostratified columnar epithelium that is similar to bronchial epithelium and surrounded by bundles of smooth muscle (Fig. 4B).
The postoperative course was uneventful, and the patient was discharged on the 5 th day after the operation.
Discussion
Cystic lesions of the gallbladder are rare and generally consist of heterogeneous disease groups including acquired, neoplastic, or congenital cysts. The majority of gallbladder cysts are acquired, and congenital cysts are rare (6). There are several hypotheses to explain the causes of congenital cysts of the gallbladder: [1] anomalies occurring early in embryonic life may result in the formation of aberrant vesicles; [2] diverticula may be developed from incomplete or disturbed resolution of the solid stage; and [3] a true Luschka's duct originating in an aberrant duct resembles a hepatic bile duct and is found in the outer coat of the gallbladder (7).
Hence, a ciliated foregut cyst occurs as a result of abnormal budding and pinching of the tracheobronchial tree in about the fifth week of intrauterine life. Further, a ciliated foregut cyst is an uncommon developmental anomaly that usually develops above the diaphragm and is thought to be quite rare below the diaphragm (1).
Most foregut cysts below the diaphragm are found in the liver and are known as ciliated hepatic foregut cysts; extrahepatic cases are extremely rare (1). There are previous reports of cystic lesions that were lined with ciliated columnar epithelium in which the cyst was well-circumscribed, thin, and smooth (12345). In the previous five cases, the ciliated foregut cyst of the gallbladder was found to protrude into the lumen of the gallbladder on US (12345). Intramural unilocular cysts containing thick mucinous fluids ranging in size from 1.1 to 3.0 cm were present (12345). Three cases were located on the fundus of the gallbladder, whereas one was on the cervix, and yet another was on the body (1234). Similar to previous reports, our case was located on the fundus of the gallbladder in the form of a 2.2-cm, well-defined, smooth, and protruding cystic lesion with a thin wall. Muraoka et al. reported that their cyst contained hyperechoic foci, which might mimic a malignant tumor (1). Our case also showed hyperechoic content within the mass on the US and high Hounsfield units on non-enhancing CT, which was correlated with the milky fluid with horny debris admixture on the histopathologic findings.
Previous reports indicate that the ciliated foregut cysts in the liver are not enhanced after the injection of contrast material (8). In another case, a study of the gallbladder found that no enhancement was seen for the same finding of a contrast-enhanced CT (5). Similarly, our case showed no enhancement.
It has been reported that neoplastic cysts of the gallbladder have malignant potential (9). However, it is often difficult to distinguish a ciliated foregut cyst from a neoplastic cyst when performing. Moreover, it is difficult to predict whether ciliated foregut cysts of the gallbladder will become malignant. As in our case, a cholecystectomy should be considered for comparison of the differential diagnoses of congenital vs. neoplastic cysts of the gallbladder. Also, the computed tomographic arteriography (CT-A) may provide more precise information as to whether the tumor is cystic or solid, and is recommended when malignancy cannot be excluded (1).
In summary, a ciliated foregut cyst of the gallbladder is rare and usually benign. Most cases were well-defined and had small mass, with no or slight enhancement on CT scans. Therefore, the radiologist should consider the possibility of a ciliated foregut cyst in the differential diagnoses of patients with a cystic lesion in the gallbladder.

 XML Download
XML Download