

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Snapping hip syndrome is characterized by an audible snapping hip on flexion and extension of the hip during exercise or with the normal activities of daily living (1).
Snapping hip syndrome is generally diagnosed by directly listening to the clicking sounds that are generated during the repeated flexion and extension of the hip or by palpating abnormal movement, and tenography (2), sonography and/or MR imaging have occasionally been used. The sonographic findings of the internal and external types of snapping hip syndrome had recently been reported (345).
In this current study, we described the MR imaging findings of external snapping hip syndrome in 16 patients with 22 snapping hips.
Materials and Methods
We retrospectively reviewed the MR images of 16 patients with 22 snapping hips, and we obtained and assessed the electronic charts of these patients at outpatient orthopedic clinics from 1998 to 2003 and all these patients had the clinical diagnosis of external snapping hip syndrome. The diagnosis of snapping hip syndrome had been made by directly listening to the clicking sounds during physical examination or by palpation by orthopedic surgeons. The clicking sound was assessed with the patient lying down in the lateral incumbent position with the affected hip joint on the top, the knee joint was extended under the condition that a sand bag was placed the opposite pelvis and so the affected extremity undergoes varus while the tension of the iliotibial band was maintained when repeating the flexion and extension of the hip joint.
The control group was composed of 21 age matched patients (41 hips) with unilateral hip pain and who underwent hip MR. These patients were randomly selected from a larger number of patients who underwent MRI from 1998 to 2003 and who were without evidence of clinically proven snapping hip, and then the hips were divided into two groups of hips: 1) the painful symptomatic side of the hips (20 hips) and 2) the asymptomatic side of the hips (21 hips).
Our institutional review boards didn't require their approval or informed patient consent for retrospective study of the case records and MR studies.
All the patients underwent MR imaging (1.5T system, Philips, Gyroscan NT, Eindhoven, The Netherlands.) of the hip. The imaging sequences include the coronal T2-weighted image (TR/TE: 3800 ms/ 90 ms), the axial T1-weighted image (TR/TE: 500 ms/ 20 ms), the axial fat saturated T2-weighted image and the axial T2-weighted image of the hip. The imaging parameters included a 180 mm field of view (FOV), 4 mm slice thickness, a 0.5 mm gap, a 256×196 matrix and two or three excitations. The MR image of the unaffected hip was also obtained: the T2-weighted axial image with a 180 mm FOV and a 330 mm FOV.
The MR images of snapping hip syndrome were evaluated by the thickness and contour of the iliotibial band and the gluteus maximus, the bone marrow of the hip joint and other associated pathology of the hip joint like a labral tear, the presence of loose bodies and bursal abnormalities. The thickness of the iliotibial band and the anterior border of the gluteus maximus were measured separately at the level of the femoral greater trochanter on the axial T1 weighted image. Both hips were compared on the axial and coronal images with a 330 mm FOV, and the structure of the affected hip was observed in more detail on the axial image with a 180 mm FOV. Abnormality of the bone marrow, the presence or absence of bone marrow edema (increased signal intensity on the T2-weighted image), joint effusion and the presence or absence of bursitis were evaluated on the T2-weighted images with or without fat suppression. Two musculoskeletal radiologists analyzed the images and the clinical findings.
Statistical analysis was done using chi-square tests and independent sample T tests. A p value of less than 0.01 was considered statistically significant.
Results
The mean age of the patients with snapping hip syndrome was 38 years (range: 15 to 61 years; 11 men and 5 women) and the ages of the control group ranged from 19 to 61 years (mean: 39 years; 15 men and 6 women). Six cases exhibited bilateral hip snapping. The mean duration of the symptom was 42 months (range: 14 to 70 months). All the patients with snapping hip syndrome displayed audible snapping, which was well correlated with hip pain. None of the cases had a past history of fracture or surgery in the hip joint area.
The causes of the hip pain for the control group were confirmed as follows: avascular necrosis (5 hips), labral tear (7 hips), tendinitis (1 hip), osteitis (2 hips), synovitis (2 hips) and idiopathic (3 hips); 1 hip on the symptomatic side was excluded from the analysis due to being in a post-operative state after total hip replacement.
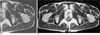
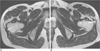
The MR imaging features of snapping hip syndrome included thickening of the iliotibial band and/or thickening of the anterior band of the gluteus maximus in nineteen hips (86%) (Figs. 1, 2, 3), and wavy contour of the iliotibial band or the anterior band of the gluteus maximus in ten hips (45%) (Fig. 4). Summarizing the imaging finding of the unaffected hip, the range of thickness of the iliotibial band and the anterior border of the gluteus maximus was 1.5 - 2 mm. On the other hand, those structures in the hip that generated snapping hip syndrome were thickened and they were measured to be over 2 mm (iliotibial band : 2.8 mm - 5.5 mm, gluteus maximus: 2 mm - 6.7 mm). Among them, three cases were thickened to over 5 mm. The difference of thickness of the iliotibial band and the anterior border of the gluteus maximus was statistically significant (Table 1). The mean thickness of the thickened iliotibial band and the anterior border of the gluteus maximus for the patients with snapping hip syndrome was 3.8 and 3.7 mm, respectively.
The associated findings were fibrosis in the space between the greater trochanter and the anterior band of the gluteus maximus in 12 hips (55%), bone marrow edema in the greater trochanter in one hip (4%), joint effusion in ten hips (45%), and trochanteric bursitis in two hips (9%). The fibrosis in the space between the femoral greater trochanter and the iliotibial band or the anterior border of the gluteus maximus was seen as low signal intensity on both the T1- and T2-weighted images and intermediate to high signal intensity on the fat-suppressed T2-weighted image (Fig. 5). Most of the snapping hips (11 hips) were detected in the patients with a thickened iliotibial band and/or gluteus maximus and one case showed fibrosis without the thickening of the above mentioned two structures. These associated findings were not statistically significant.
Surgical treatment was done via Z-plasty in 5 patients with 6 hips that were resistant to conservative treatment.
Discussion
The causes of the snapping hip syndrome include two entities: the intraarticular type and the extraarticular type. The causes of the intraarticular types of snapping hip syndrome are a loose body, labral tear, synovial osteochondromatosis etc. The most common cause of the extraarticular external type of snapping hip syndrome is the iliotibial band (or iliotibial tract) sliding over the greater trochanter. Any conditions that cause an abnormal thickening of the iliotibial band or an abnormal relaxation of gluteus maximus muscle may be the responsible for snapping hip syndrome. The internal type of extraarticular snapping is the iliopsoas tendon slipping over the iliopectineal eminence. Other causes include iliopsoas bursa slipping of the iliofemoral ligament over the femoral head and slipping of the long head of the biceps femoris tendon over the ischial tuberosity (1678910)
Mayer insisted that the major factors of snapping hip syndrome were abnormality of the fascia lata that forms the catch back of the posterior greater trochanter, unusual prominency of the trochanter, abnormal relaxation of the gluteus maximus muscle and irregularities of the acetabulum (8). In addition to the fascia lata being the cause, there has been a reported case that developed snapping hip syndrome due to a band of fibrous tissue that corresponded to a portion of the gluteus maximus muscle. Such fibrosis may be developed due to repeated intramuscular injection of antibiotics and analgesics or during the treatment process of chronic illness, yet blood vessel injury may develop even after one injection (9). In our study, there were no cases that developed due to repeated intramuscular injection of antibiotics or analgesics. The major causes of external snapping hip syndrome are currently thought to be the gluteus maximus and the iliotibial band in most cases (6789). Similarly in our study, the cases showing the thickening of the anterior border of the gluteus maximus and the iliotibial band simultaneously was 55%, and the percent of cases with thickening of the gluteus maximus or the iliotibial band only was 86 %, and 55 %, respectively.
Snapping hip syndrome is developed more frequently due to the tight iliotibial band (6). However, the result of our study showed that 45% of the cases showed the wavy contour of the affected iliotibial band, as compared with contralateral side. This finding may be undetected on unilateral hip MR imaging and it has not been previously reported in the medical literature. Mayer et al. (8) mentioned that abnormal relaxation of the gluteus maximus may be a possible cause of snapping hip syndrome. We think a wavy contour of the iliotibial band or the anterior border of the gluteus maximus is the cause of snapping hip syndrome. Therefore, we recommend MR images of both hips for making the diagnosis of the snapping hip syndrome.
It has been reported that the hip pain in patients with snapping hip syndrome patients is highly associated with greater trochanteric bursitis, and bursitis has been considered to be a cause of snapping in some cases (111). However, in our study, the hips of only two patients showed the finding of accompanying bursitis; hence, it appears that the association of greater trochanteric bursitis with snapping may be low.
There have been several reports that have focused on the sonographic findings of extraarticular snapping hip syndrome. The reported sonographic findings were tendinitis, bursitis, synovitis or local tenderness over the course of the tendon and an asymmetric tendon around the hip (the iliopsoas tendon, the rectus femoris tendon and the iliotibial band). Several recent reports that performed dynamic sonographic study identified the abnormal displacement of the iliopsoas tendon or sudden abnormal jerky movement of the iliotibial band/gluteus maximus muscle over the greater trochanter (34). However, sonography may not identify the underlying causes of the snap for the patient who cannot reproduce the snap during sonographic examination. Sonography cannot evaluate the intraarticular causes of snapping hip syndrome.
Faraj et al. (6) reported that for 10 patients who underwent successful surgery to correct tight and symptomatic iliotibial band snapping, MRI and CT were performed in 6 cases and 4 cases, respectively, and abnormal findings were not detected in all the cases. Choi et al. (4) reported only one abnormal finding of iliotibial band thickening on the MR images of four patients with external snapping hip syndrome. However in our study, abnormal findings of the anterior border of the gluteus maximus and iliotibial band were detected in the majority of cases, except for two cases. Among these two cases, one case showed normal finding of the MR image and another case showed fibrosis between the femoral greater trochanter and the iliotibial band. Our MR protocol with the T2-weighted axial images of both hips and using a small FOV is important to increase the rate of detecting abnormal findings of snapping hip syndrome, as compared with that of the unaffected hip. Axial images with a large FOV were also helpful for increasing the sensitivity to detect lesion in the affected hip. In our study, this protocol was able to reduce the false negative findings of snapping hip syndrome.
For painful snapping hip, conservative treatment such as rest, stretching, exercise and oral anti-inflammatory drugs are often enough to alleviate the symptoms. But for patients who resistant to conservative treatment, an operative procedure is required and several good results have been reported after operation via Z-plasty (167). In our study, surgery with Z-plasty was performed on 5 patients, and good outcomes were obtained.
This study is limited by the fact that our data was retrospectively analyzed for making the clinical diagnosis of external snapping hip syndrome. As most of the patients were managed conservatively, there was a lack of surgical correlation. Nevertheless, our imaging findings did correlate with the definite clinical diagnosis of the external snapping hip syndrome. Also, the absence of a clinical snapping hip was not confirmed in the control group, but the history of the painful hip in the control group did not include the clicking sounds of the hip.
In conclusion, MR imaging is a sensitive imaging modality for identifying the cause of the external snapping hip. The major MR imaging features were the thickening of the iliotibial band and the anterior border of gluteus maximus, and the wavy contour of these structures.




 XML Download
XML Download