

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Osteoarthritis of the atlantoaxial joints has a prevalence of between 5% and 18%. Only a minority of the patients with osteoarthritis of the atlantoaxial joints become symptomatic and suffer from severe suboccipital pain. Most often, these patients can be successfully treated using conservative methods. However, some of these patients require surgical treatment (1).
To the best of our knowledge, there have been no reports on abnormality of the venous circulation at the craniocervical junction and its clinical implications in patients who suffer from degenerative osteoarthritis of the C1-C2 facet joint with atlantoaxial subluxation.
We have a keen interest regarding the hemodynamic alterations of the cervical venous plexus in these patients as there was a significant dilatation of the suboccipital cavernous sinus, the internal and external vertebral venous plexuses and the deep cervical veins observed on our patient's initial MR images. Furthermore, follow-up MR study revealed a significant decrease of the enlarged venous plexuses and deep cervical veins after occipitocervical reduction and fusion.
It is also important to consider that the significant dilatation of the cervical venous plexus might be the cause of the vigorous bleeding encountered when dissecting the venous plexus surrounding the C2 nerve root and immediately on top of the C1 lateral mass (2) during surgery.
Case Report
A 52-year-old woman was hospitalized for surgical treatment due to severe incapacitating occipitocervical pain and a marked decrease of cervical rotation, and she'd had these symptoms for about the previous 8 years. The patient suffered severe occipitocervical pain when flexing and rotating her head, and this was exacerbated by laughing, coughing and straining. In addition to the headache, the patient experienced nausea, vomiting, anorexia and dizziness when standing and these symptoms gradually disappeared when the patient was lying down. There was no history of trauma and she had previously received conservative treatment for her symptoms at a private clinic. However, her occipitocervical pain did not respond despite the treatments. Her occipitocervicalgia persisted and was further aggravated over the last several months. The patient was referred to our department by a primary care provider.
On physical examination, cervical rotation to the right was painful and markedly limited. Any neurological deficits were not present. The laboratory studies (C-reactive protein, rheumatic factor, ESR) that were carried out to rule out systemic inflammatory disease were normal.
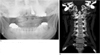
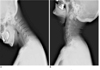
An open-mouth radiograph (Fig. 1A) and a CT scan (Fig. 1B) showed osteoarthritis of the right atlantoaxial facet joint with narrowing of the joint space, subchondral sclerosis, peripheral osteophyte formation and erosions of the joint, as well as left lateral listhesis of C1 on C2. There was a subluxation of C1 on C2 on the flexion and extension lateral radiographs of the cervical spine (Fig. 2). A bone scan revealed a focal uptake unilaterally at C1-C2. There was significant dilatation of the suboccipital cavernous sinus, the internal and external vertebral venous plexuses and the deep cervical veins on the axial gradient-echo T2*-weighted MR images (Fig. 3A) and the contrast-enhanced spin echo T1-weighted MR images (Fig. 3B). Occipitocervical reduction and fusion (Fig. 4), which is a common method of dealing with upper cervical spine instability, was performed under general anesthesia. Immediately after the surgery, the patient's pain dramatically decreased, although her wound pain lasted for 10 days. A follow-up MR study revealed a significant decrease of the enlarged venous plexuses and deep cervical veins (Fig. 5). She was free of occipitocervical pain within 3 months following the surgery.
DISCUSSION
This is a successful case of surgically managing atlantoaxial degenerative osteoarthritis with subluxation of C1 on C2, the accompanying severe occipitocervicalgia and the significant dilatation of the suboccipital cavernous sinus, the internal and external vertebral venous plexuses and the deep cervical veins. We radiologically identified degenerative osteoarthritis of the atlantoaxial facet joint with instability. We noticed that these dilated cervical veins could not be seen any longer and the patient had complete relief of her pain after the occipitocervical reduction and fusion. The venous dilatation of the craiovertebral junction was best assessed on the axial T2*-weighted gradient echo sequences and the T1-weighted (fast spin echo (FSE)) images with contrast enhancement.
When considering this case, our two main questions were: Why did her pain develop and how can it be cured? Epidural venous enlargement may occur in a variety of lesions, including vascular malformations and venous obstructive lesions (3). An instance of greatly enlarged craniocervical epidural veins after craniectomy has been recently reported in the literature (4). However, there have been no reports of a correlation between degenerative osteoarthritis of the atlantoaxial facet joint and instability and severe occipitocervicalgia.
Anatomically, the C1-C2 region is related to the meeting point of the superior and inferior suboccipital triangles (5). The venous cushion, which surrounds the atlantal part of the vertebral artery at the floor of the superior suboccipital triangle, has been termed the suboccipital cavernous sinus by Arnautovic et al. (5). The inferior suboccipital triangle contains the beginning of the twofold posterior external vertebral venous plexus, that is, 1) the vertebral venous plexus surrounding the upper cervical part of the vertebral artery and 2) the deep cervical veins. All the components are connected to the suboccipital cavernous sinus in the superior suboccipital triangle (5). The suboccipital cavernous sinus is reported to contain an ampulloglomerular organ that is thought to be important for pressure regulation (6).
Yousry et al. (7) described that the vulnerability of the dura at the C1-C2 level to shear stress could be related to the mobility of this segment, which is higher than all the other segments, and to the fact that the dura lacks bony support over a distance that is longer than all the other intervertebral spaces.
According to the Monro-Kellie rule, the cerebrospinal fluid (CSF) volume fluctuates with the intracranial blood volume (8). In the presence of an intact skull and thus a constant intracranial volume, the the Monro-Kellie hypothesis dictates that a decrease of the CSF volume leads to compensatory vasodilatation in the brain and meninges (9). The close connection between both the intracranial and the intraspinal venous systems makes it probable that dilatation of the cranial meninges will be associated with dilatation of the intraspinal venous system, and namely the internal vertebral venous plexus. Although the internal venous plexus is continuous throughout the spinal canal, it is noteworthy that the dilatation is always most prominent at the C1-C2 level. This increased distensibility could be related to a larger venous plexus and reduced bony support at the C1-C2 level (10). Mokri et al. (9) found that intracranial hypotension is more likely to be the result of a decrease in the CSF volume than from a decrease in the CSF pressure. Therefore, he introduced the term CSF hypovolemia.
On the basis of the above information, we hypothesized that mechanical stress on the C1-C2 region that's caused by atlantoaxial instability might result in hemodynamic alteration of the veins of the suboccipital and upper cervical area, and this all shows as venous dilatation of the craniocervical junction. When a blood-pressure cuff is applied and inflated on the upper arm, we can see the 'obstructive' engorgement of the venous vessels on the dorsum of the hand. When the cuff is then gradually deflated, the venous dilatation disappears. In a similar manner, atlantoaxial instability might act just like a 'blood-pressure cuff' at this area and cause 'obstructive' venous dilatation of the craniocervical junction. The distended spinal veins might cause an alteration of the intracranial CSF pressure or volume-intracranial hypotension, resulting in dilatation of the cranial meninges and occipitocervicalgia. Moreover, in our case, the dilated venous plexus significantly decreased in dimension and it returned to normal on the postoperative MR images, which paralleled the improvement of the patient's occipitocervical pain, and this was the result of correcting the atlantoaxial instability. In accordance with the Monro-Kellie hypothesis, we thought that our patient's improvement was most likely due to correcting the previous intracranial CSF hypovolemic condition.
To sum this up, degenerative osteoarthritis of the C1-C2 facet joint with atlantoaxial subluxation can cause hemodynamic alteration of the venous circulation (venous enlargement) at the craniocervical junction, and this causes occipitocervical pain. This can be corrected by occipitocervical reduction and fusion.
In conclusion, the severe occipitocervical pain in this case of degenerative atlantoaxial osteoarthritis and instability could be related to the venous dilatation of the craniovertebral junction, and this can be best assessed on the axial gradient-echo T2*-weighted and contrast-enhanced T1-weighted MR images.



 XML Download
XML Download